Observation
Footwear –
- observe for wearing pattern on the shoe.
- cavus feet – wear pattern on the outer side of the shoe.
- planovalgus foot – wear pattern on the inside of the shoe (can happen due to tibialis posterior dysfunction or coalition).
- equinus foot – wear on the front of the shoe.
Gait
Foot Progression Angle –
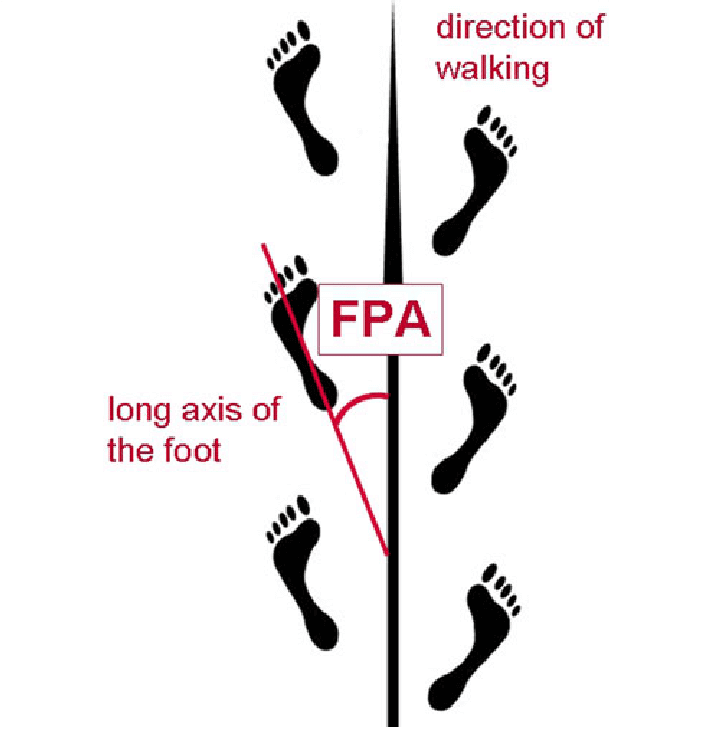
- angle of foot from a horizontal line when walking. Most people will walk with the foot in slight external rotation.
- If someone is walking with the foot parallel to the line, it is neutral foot progression angle.
- If someone is walking with the foot in internal rotation, then it is called negative foot progression angle. This is not normal. Most likely cause is persistent femoral anteversion.
- Antalgic gait – decreased stance phase and decreased stride length.
- Cavus gait – patient walking on the outside of their feet.
- planovalgus gait – patient walking on the medial side of their feet.
- High step gait – happens in foot drop.
- reduced toe off during gait – happens in hallux rigidus.
Inspection (standing)
Front
- look at overall spinal posture, any varus / valgus at knee and foot posture.
- From the front if one can see too much of the heel, it suggests a cavovarus deformity. This is called Peekaboo sign.
- Also look at the arch of the foot.
- look for any calf or thigh muscle wasting, previous incisions or scars.
* look for any toe deformity – Bunion, Hallux valgus / varus.
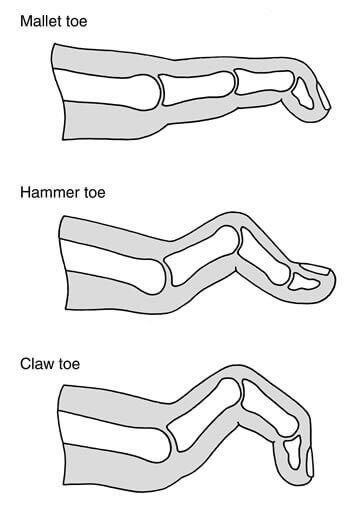
Look for any lesser toe deformity –
- Claw toe (MTP in hyperextension, PIP in flexion, DIP in flexion)
- Hammer toe (MTP in extension, PIP in flexion, DIP in slight extension),
- Mallet toe (DIP in flexion).
- Observe the webspaces – look for any signs of fungal infection. Look for any naevus. Sometimes there can be a melanoma present.
Lateral View
- look for any fullness around ankle, any muscle wasting in calf and anterior compartment of the leg.
- look at the arch whether it is flat or not.
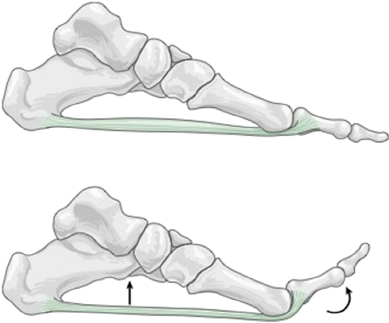
* If the arch is flat in standing, then in the same standing position, passively dorsiflex the big toe.
In a flexible flat foot, with dorsiflexion of big toe, the arch will form. This is called Jack’s Test.
Look from Behind
- observe spine – look for naevus, tuft of hair.
- look for hams, calf wasting. In Charcot Marie tooth, there may be a cavus foot with calf muscle abnormality.
- Also look for any fullness around the achilles, achilles bursitis, insertional tendinopathy.
- * Alignment of hindfoot – normally the heel is in 5° of valgus.
- * How many toes can one see from this view? Normally one should see one and a half toe. More than 2 toes is a sign of a planovalgus foot. One reason can be tibialis posterior dysfunction. This is also called Too many toes sign.
- With tip toe position, the heel will normally go into varus.
Sole of foot *
- observe the arch
- normal weight bearing occurs at heel, 1st MTP joint and 5th MTP joint.
- Increased weight bearing over the 2nd or 3rd toe causes callosities on the sole of foot around the 2nd and 3rd MTP joints. This is a classical sign for transfer metatarsalgia. This means abnormal weight bearing is happening secondary to disturbed biomechanics of the foot.
Palpation
Pulses
- Dorsalis pedis
- Posterior tibial pulse
Sensation
Attribution: RSNA
- Superficial peroneal nerve –
- Deep peroneal nerve – 1st webspace
- Medial plantar
- Lateral plantar
- Sural nerve
Foot Palpation
Posterior part
- Start with tendoachilles – feel for any gap, bump, nodule. Check insertion of achilles for tenderness.
- Palpate for Posterior Impingement – behind the medial malleolus. It is seen in footballers, ballet dancers where they have an os trigonum. They are tender over the region. Forced plantar flexion of the ankle causes pain.
- Palpate lateral calcaneal tuberosity which is tender in Haglunds Deformity.
Medial side
- Palpate medial malleolus, deltoid ligament for any tenderness.
- Palpate medial plantar fascia – for plantar fasciitis.
- Tenderness over the heel is more suggestive of fat pad atrophy.
- Palpate for tibialis posterior tendon – look for pain, fullness. This is more so due to tibialis posterior dysfunction and sometimes due to synovitis of flexor hallucis longus. If it is due to FHL synovitis, then move the big toe into flexion and extension with the foot plantar flexed. In this position it would move nicely. Then do the same with foot in dorsiflexion, you would notice that the movement reduces and also that it causes a pain along the FHL tendon posterior to the medial malleolar region.
- Tenderness along the tibial nerve posterior to medial malleolar region can produce tingling in the foot on tapping the nerve. This can be due to Tarsal Tunnel Syndrome.
Front of Ankle
- Look for tenderness over ankle joint line. Palpate the medial gutter and the lateral gutter. Tenderness in this region can be due to ankle OA or sometimes osteochondral lesion.
- Fullness in medial and lateral gutter region may suggest synovitis.
Lateral Ankle
- Feel for lateral aspect and any bony tenderness over lateral malleolus.
- Feel for any tenderness over ATFL, CFL and PTFL
- Feel for any tenderness behind the lateral mallolus over peroneal tendons.
- Feel for tenderness over sinus tarsi which may be due to subtalar joint.
- Squeeze test – squeeze the calcaneum. If tender, it can suggest an insufficiency fracture of the calcaneum.
Midfoot
- Chopart Joints – Talonavicular Joint and Calcaneocuboid Joint.
- Feel for talonavicular joint. Tenderness may be due to OA. Sometimes a bump may be felt over the region which is due to an accessory navicular.
- Feel for talonavicular joint.
- Palpate mid tarsal joint.
- Palpate individual metatarsals.
Few Extra Palpation Areas
- Plantar surface of 1st MTP joint. Tenderness over medial aspect can be due to medial sesamoiditis and tenderness over lateral aspect can be due to lateral sesamoiditis.
- Tenderness over MTP joint in the presence of callosity underneath the MTP joint is positive for transverse metatarsalgia.
- Tenderness in webspace can suggest Morton’s Neuroma.
Movement
Active ROM
- Ankle dorsiflexion ~ 20°
- Plantarflexion ~ 40°
- Inversion ~ 20°
- Eversion ~ 10°
Passive ROM
Ankle – Ankle dorsiflexion and plantarflexion – to check passive DF, move the ankle into slight inversion and then move the ankle into PF and DF. This locks the chopart joints. In a case of ankle fusion, one can be misled by DF occurring at the chopart joints.
Subtalar joint – 5° of inversion / eversion or varus / valgus. Immobilise the talus by putting thumb at the talar neck region and then hold the calcaneum and move it into varus and valgus. Pain with walking on uneven surface is indicative of an issue with the subtalar joint.
Inversion – it is a combined movement that occurs at subtalar, chopart and also at midtarsal joints.
Eversion – complex movement occurring at subtalar joint and chopart joints.
Midfoot – forefoot adduction and abduction occurs at transverse tarsal joints. Fix the midfoot and the passively do these movements. Also check the hypermobility of the 1st TMT joint. This can be implicated in hallux valgus.
Hallux
- DF: 80-90°
- PF: 20-30°
- Check for movement of lesser toes as well.
Muscles and Tendons
Tibialis Anterior – causes foot DF. Check by resisting foot DF in neutral ankle or slight inversion.
Tibialis Posterior – insufficiency of this causes adult acquired planovalgus deformity. To assess this have the foot in plantar flexion and inversion. Ask the patient to hold this position and resist the inversion. At the same time palpate the tibialis posterior tendon behind the medial malleolus for pain or discomfort.
Peroneus Longus – Hold foot in slight plantar flexion and eversion. Resist the eversion movement. The peroneus longus tendon becomes prominent behind the lateral malleolus.
Peroneus Brevis – Hold foot in neutral (90° ankle) and eversion. Resist eversion. The peroneus brevis tendon can now be felt behind the longus tendon around lateral malleolar area.
Special Tests
Tarsal Tunnel Syndrome – Posterior tibial nerve divides into calcaneal branch, medial plantar and lateral plantar branches.
- Tapping the region behind the medial malleolus can cause paresthesia, burning sensation or pain in the foot in the distribution of the nerve.
- Another test is to apply constant compression over the posterior tibial nerve. It that reproduces symptoms in the foot, then it is a positive test.
- To stretch the nerve, evert the foot and then apply compression over the posterior tibial nerve. Symptom reproduction is a positive test for tarsal tunnel syndrome.
Morton’s Neuroma – It is an interdigital neuroma that usually happens between 3rd and 4th metatarsals but sometimes between 2nd and 3rd metatarsals.
- Patient generally complains of pain and burning sensation in the webspace.
- Compress the webspace using a pinch grip across the forefoot. If this reproduces symptoms then it is a positive test.
- Mulder’s click – compress the MTP joints from side to side with digital pressure on the webspace from the sole. One can usually feel a click as the neuroma is moved above or below between the two MTP joints.
Gastrocnemius / Soleus Tightness
Silfverskiold test – Ankle DF improves when it is checked in slight knee flexion and worsens when the knee is extended again. This suggests tightness of gastrocnemius.
Achilles Tear
- In prone position bent the knees to 90°. A subtle clue may be that the affected foot is slightly dorsiflexed on the affected side at the ankle due to gravity.
- Simmonds test – normally compressing the calf causes plantarflexion of the foot. If there is no plantar flexion, then it is suggested of tendoachilles disruption.
Subluxation of peroneal tendons
- Sometimes after an ankle sprain, there can be disruption of peroneal retinaculum causing subluxation of peroneal tendons.
- Palpate behind the lateral malleolus and move the foot into eversion and inversion or rotate the ankle. The tendon can be felt popping.
Hallux Deformities
- Hallux valgus – usually associated with a bunion. Assess whether it is flexible and comes to neutral passively. If so, adductor release is not needed.
- Hallux varus
- Hallux rigidus – loss of toe extension. associated with bony prominence over the dorsum of MTP joint. Passive plantar flexion usually causes pain in the 1st MTP joint.
- Grind test – grind the big toe and if this causes crepitus and pain, then it suggests 1st MTP joint OA.
Syndesmotic Injury
- Squeeze Test – squeeze the tibia and fibula over the proximal tibial region. If this causes pain around the ankle then it suggests an ankle fracture or a syndesmotic injury.
Ankle Instability
- Drawer test – firm end point -> normal ATFL.
- Soft end point or excessive translation -> ATFL injury / ankle instability.
Tibialis Posterior Dysfunction
- Too many toes sign
- Excessive calcaneal valgus when standing.
- Dropped medial arch
- To assess whether this valgus is correctable or not, do single heel raise and double heel raise test. Do a bilateral heel raise. If the calcaneus goes into varus, then it means that the tibialis posterior is functioning. To assess individual tibialis posterior, do single leg heel raise. If the heel goes into valgus, it means tibialis posterior is functioning well. Do the test 2-3 times.
Coleman Block Test – this test is done for cavo-varus foot to see if it is flexible or not and whether there is any contribution of plantar flexed first ray.
Stand with lateral foot on a block or a book. Keep the medial 2 toes off the block and observe from behind. If the deformity is flexible or if there is any contribution of a plantar flexed first ray, the heel will move into slight valgus instead of usual varus of the cavo-varus foot. This means that the deformity is flexible. This helps distinguish between plantar flexed first ray or rigid or flexible deformity of the hind foot.