Hip Osteonecrosis | Cases
Published on Jan 20, 2021
- 59 ♂
- B/L groin pain. 10/10 VAS
- Initially started on the left side like lateral hip pain. Had 2 steroid injections for lateral hip pain.
- Uses walking stick.
- Painful with weight bearing, getting in / out of car.
- No spinal symptoms.
- Recent X-ray NAD
Exam
- Antalgic gait
- Pain deep in groin
- Hip flexion limited to 90° B/L
- Minimal internal and external rotation.
- Abduction 30°
- Clinician requests MRI (to rule out any soft tissue cause as the x-ray looks reassuring)
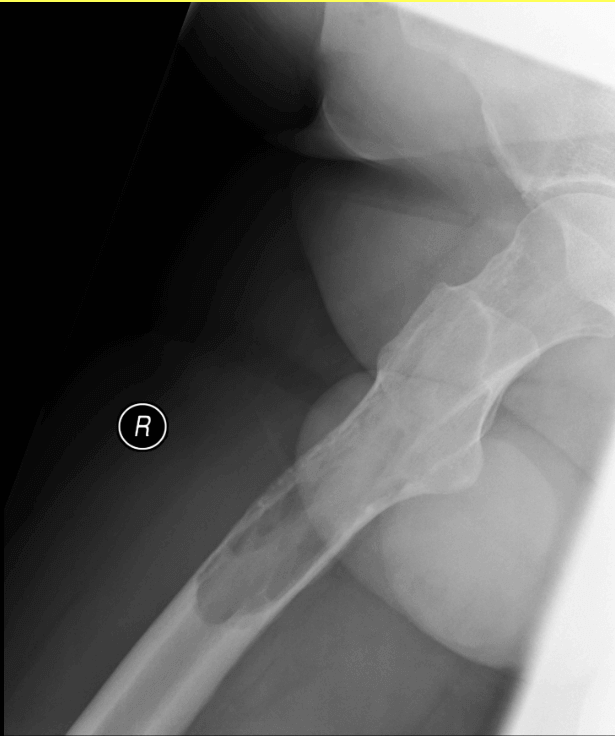
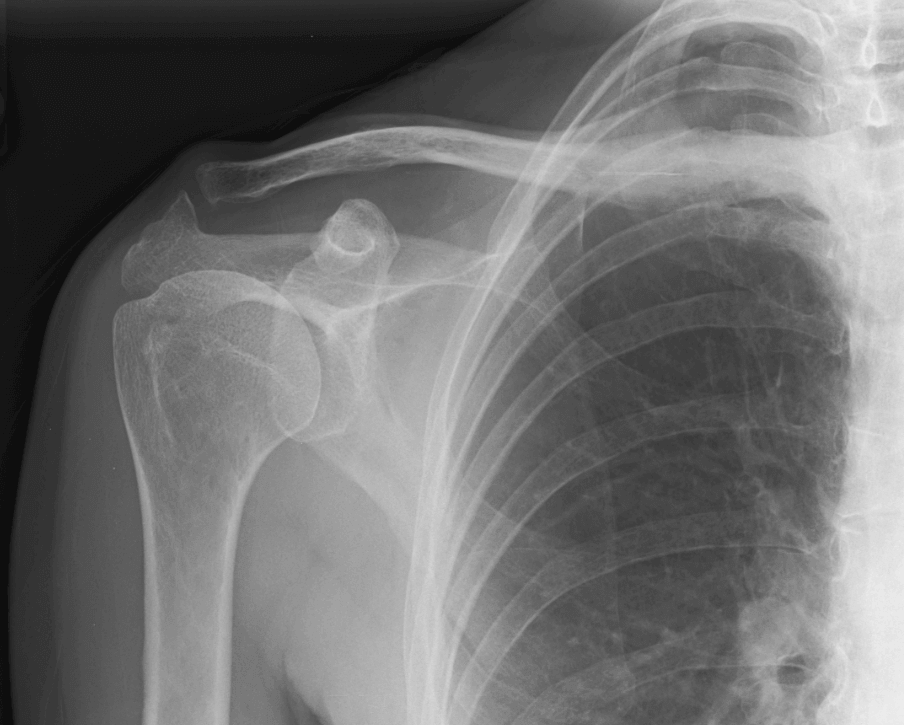
X-ray
The joint spaces are preserved. Minimal degenerative change. No focal bone lesion.
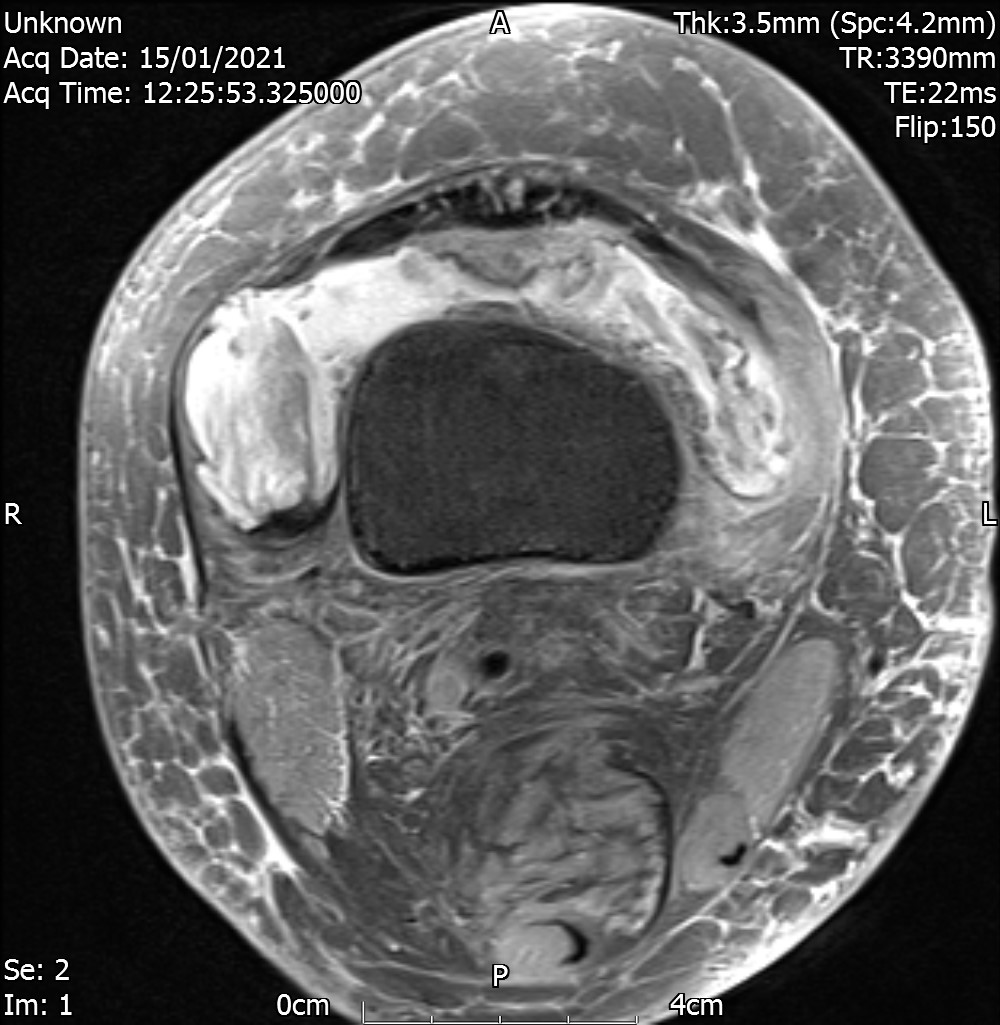
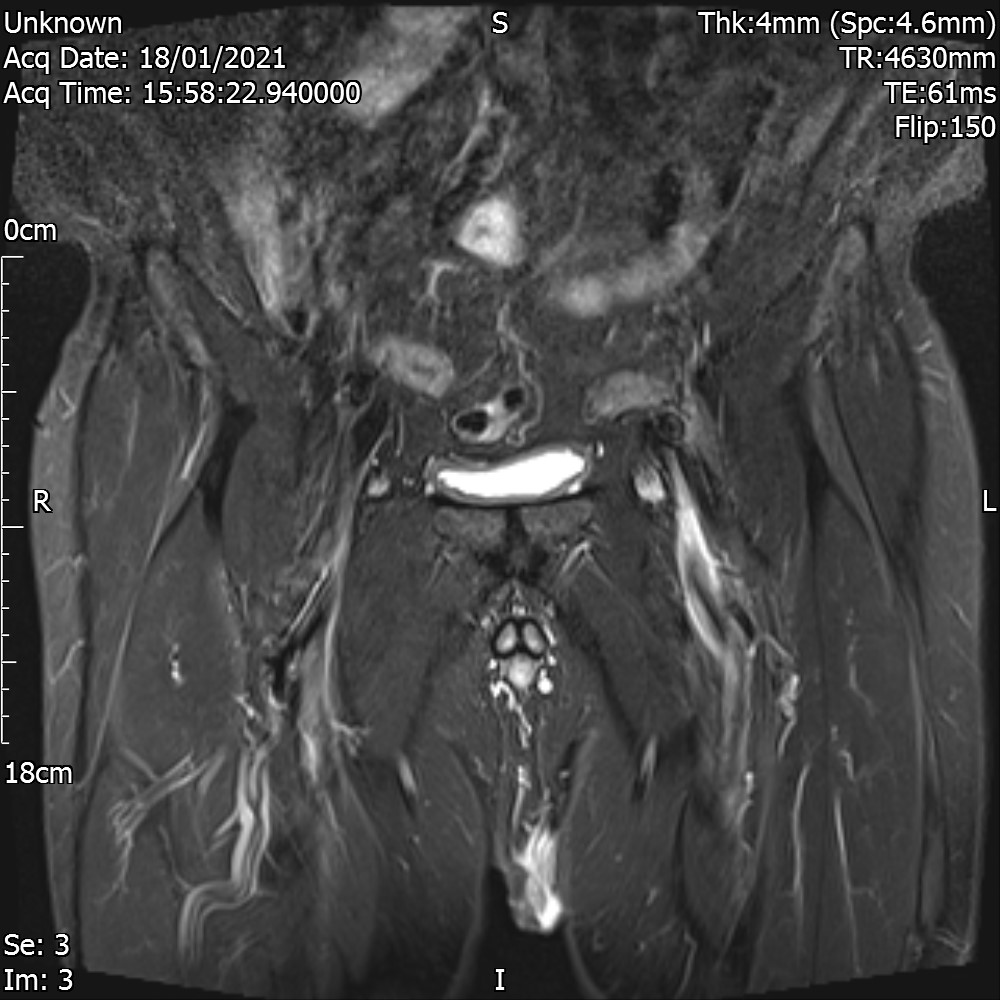
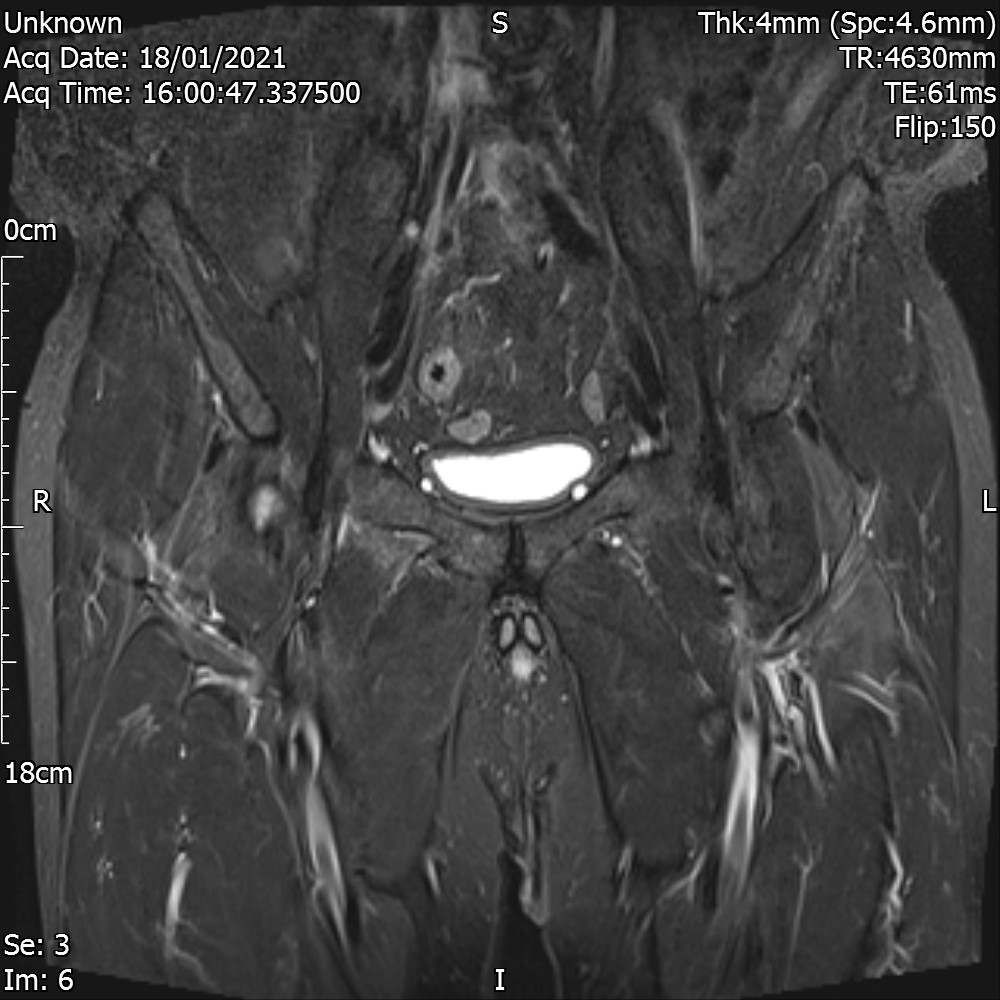
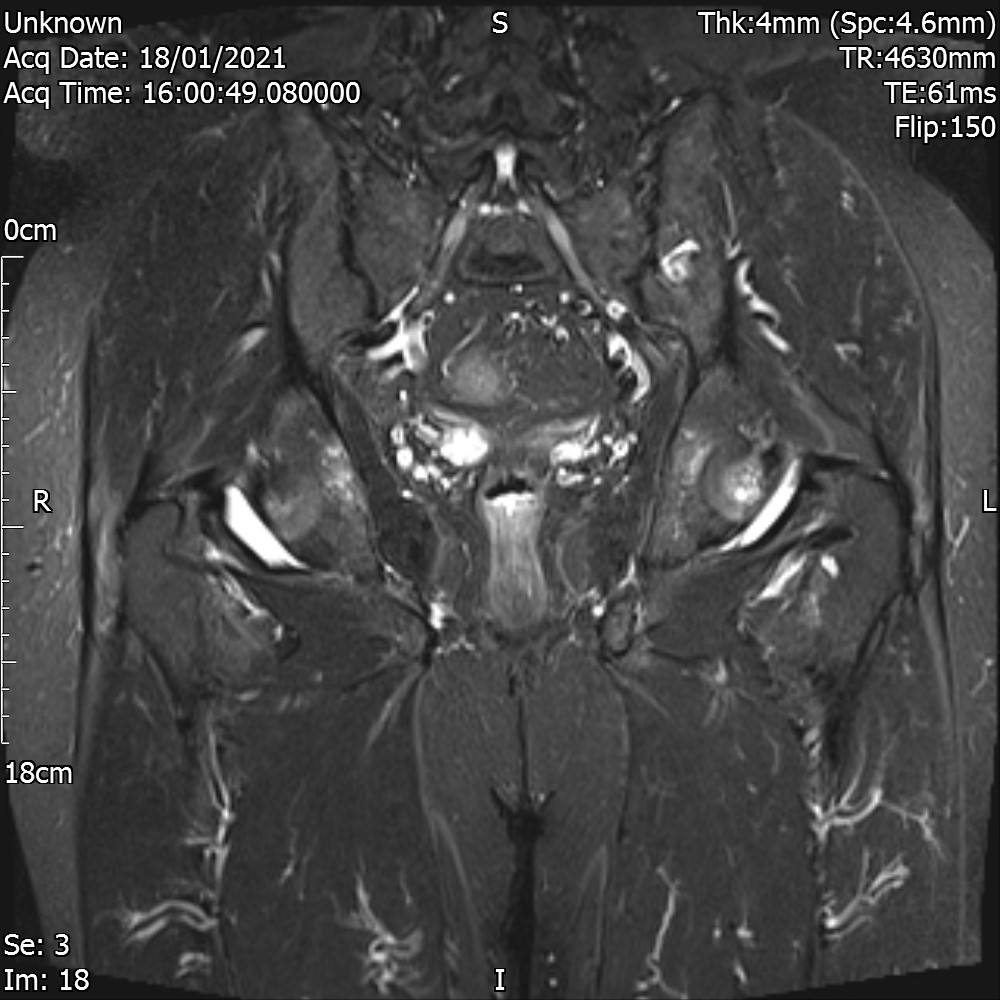
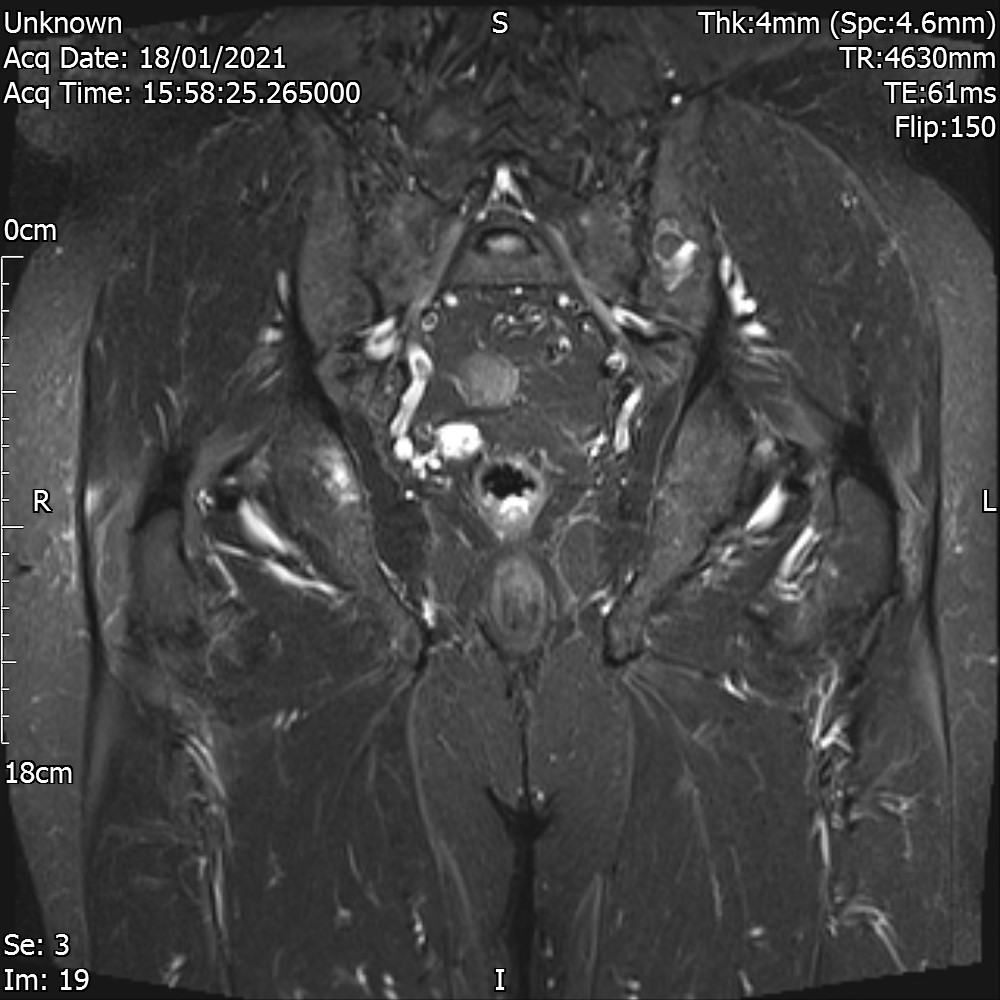
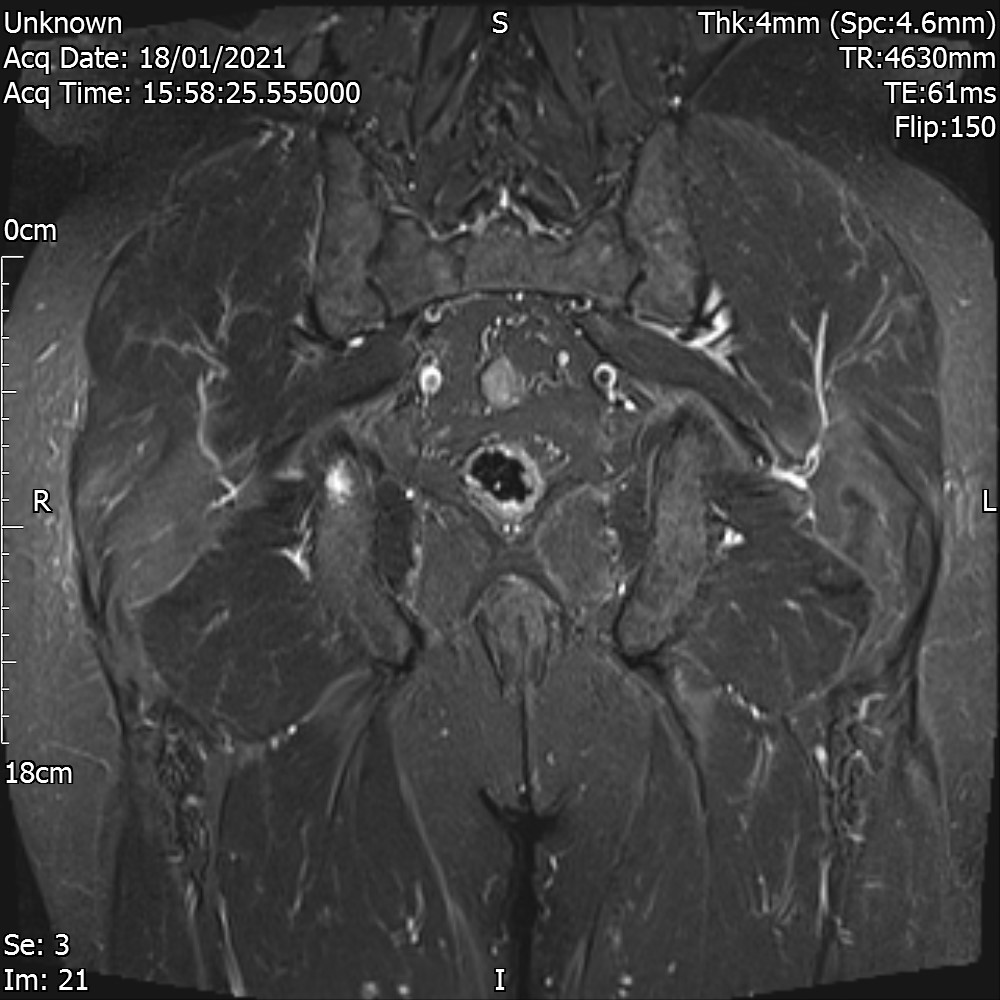
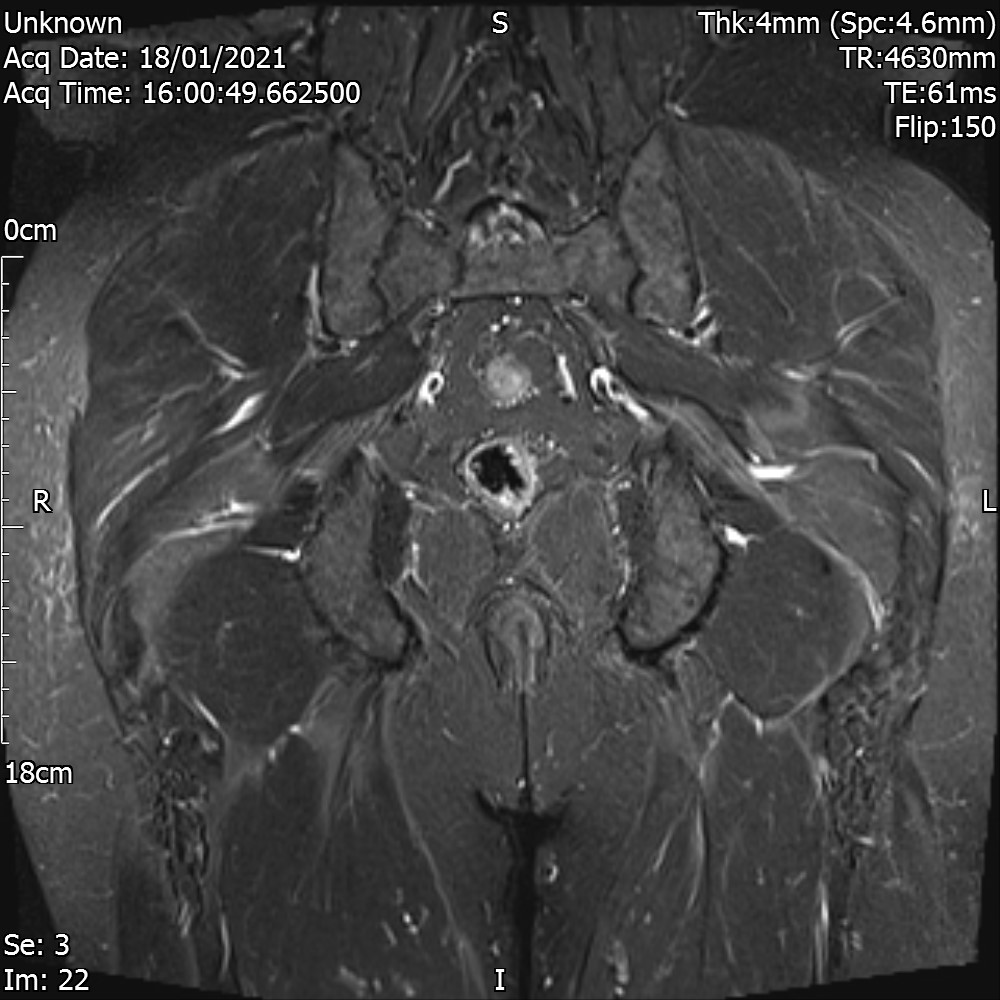
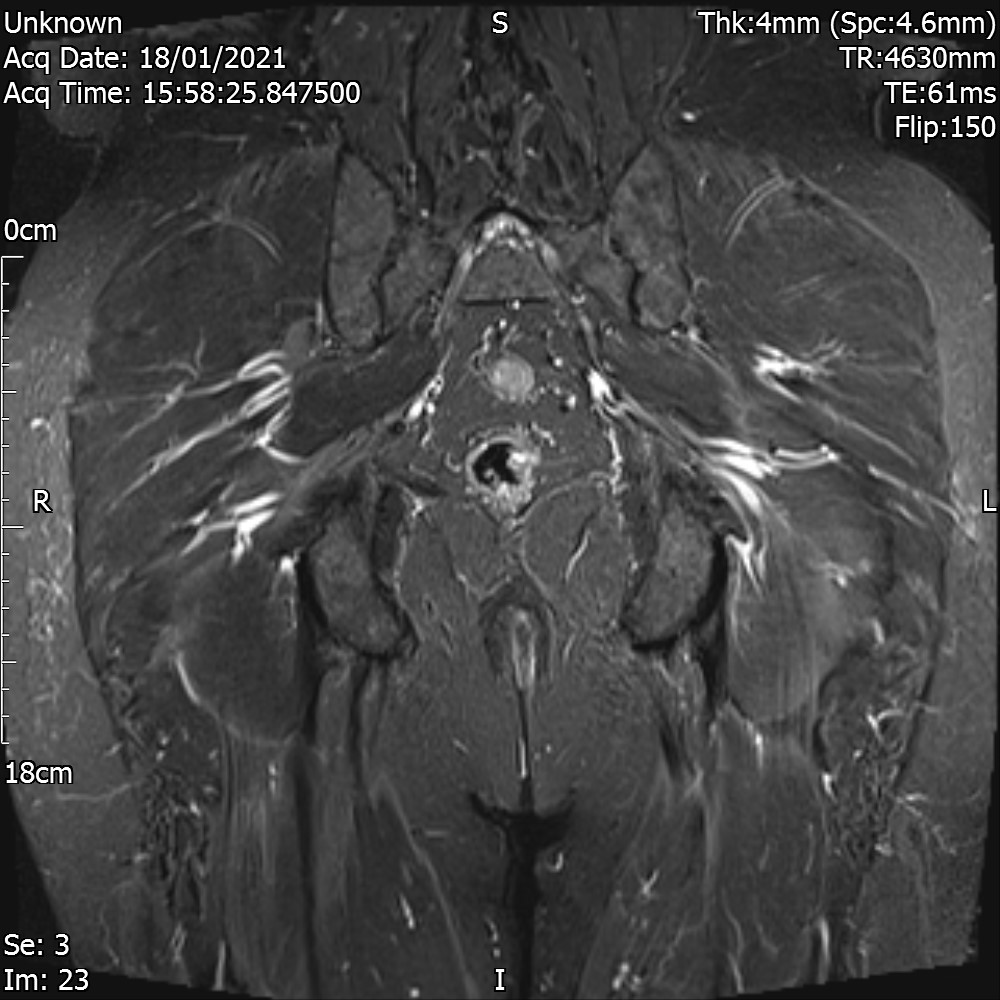
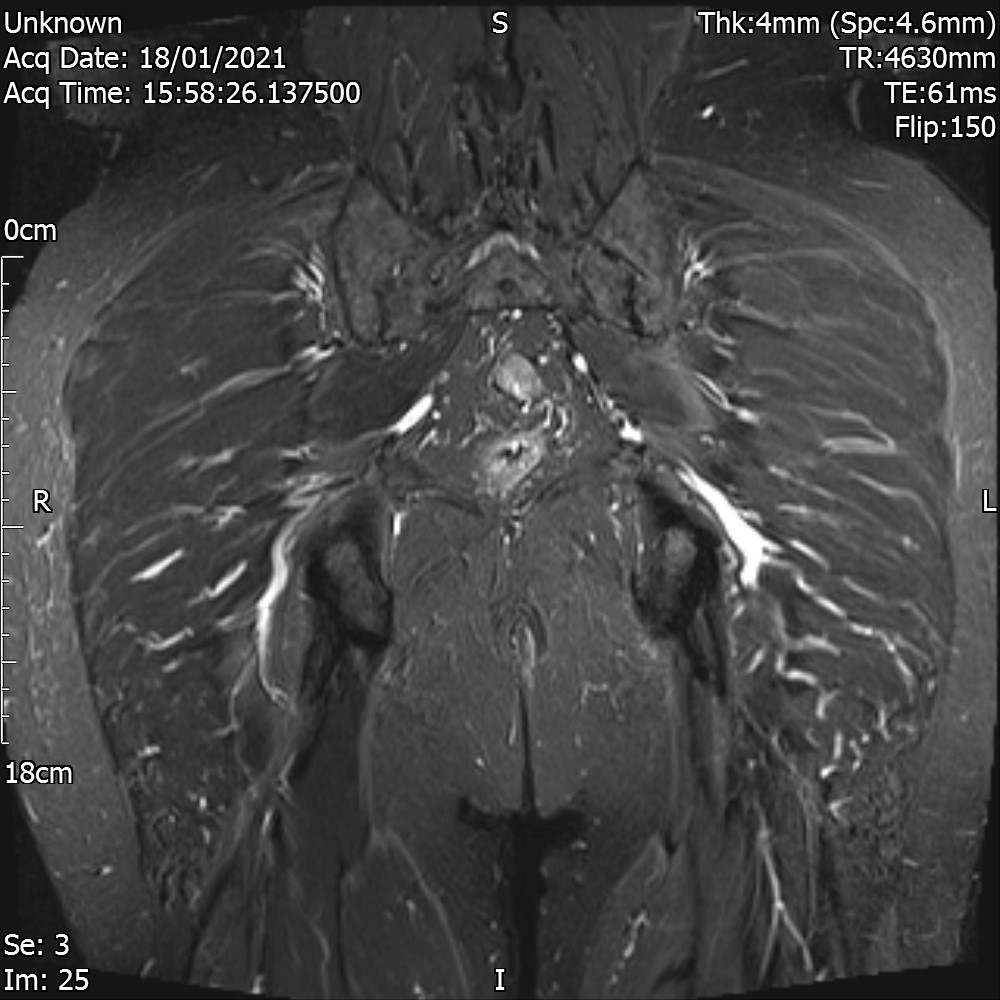
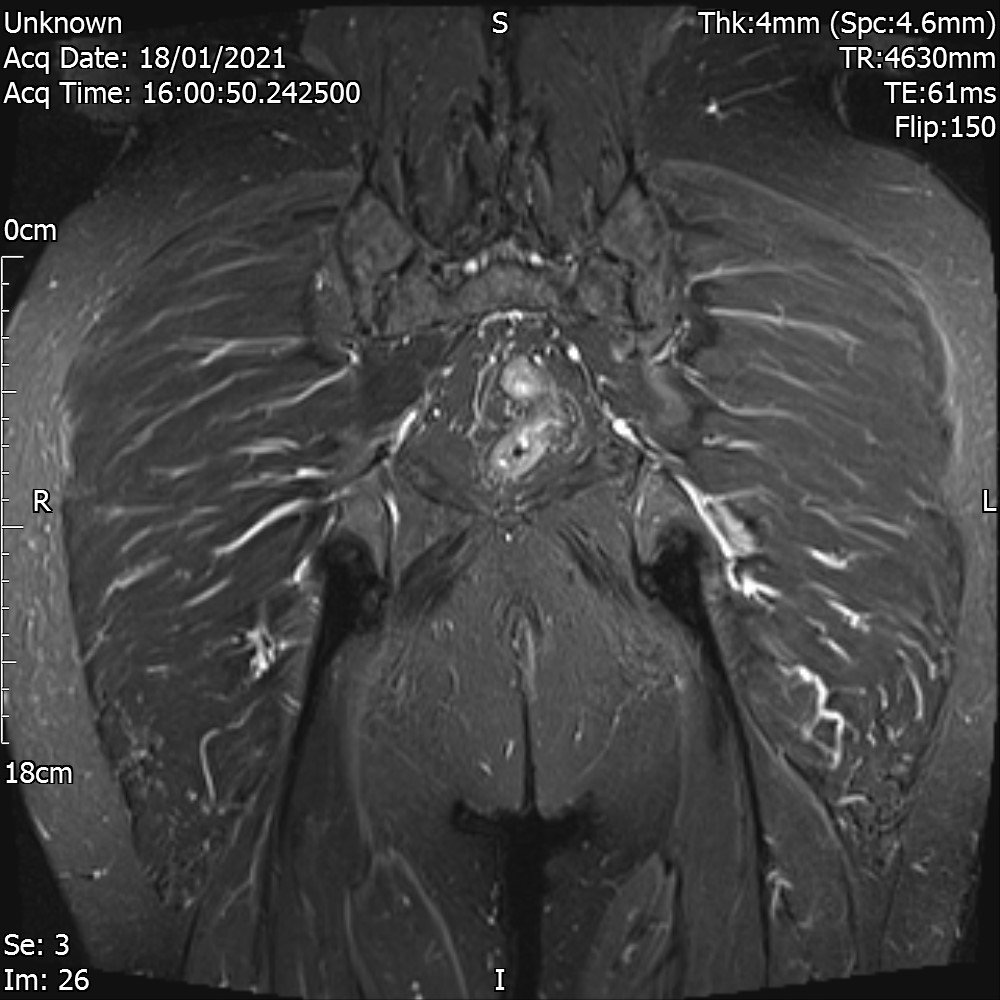
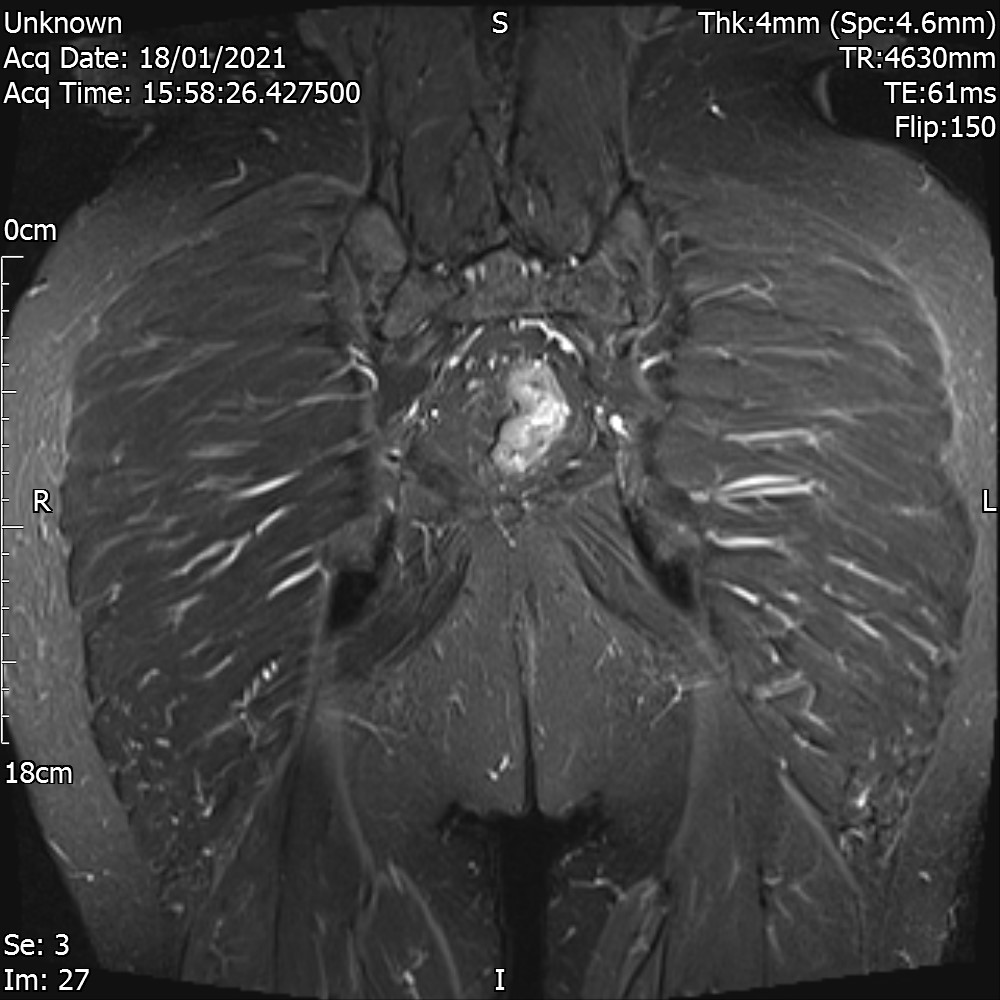
MRI
Coronal Trim



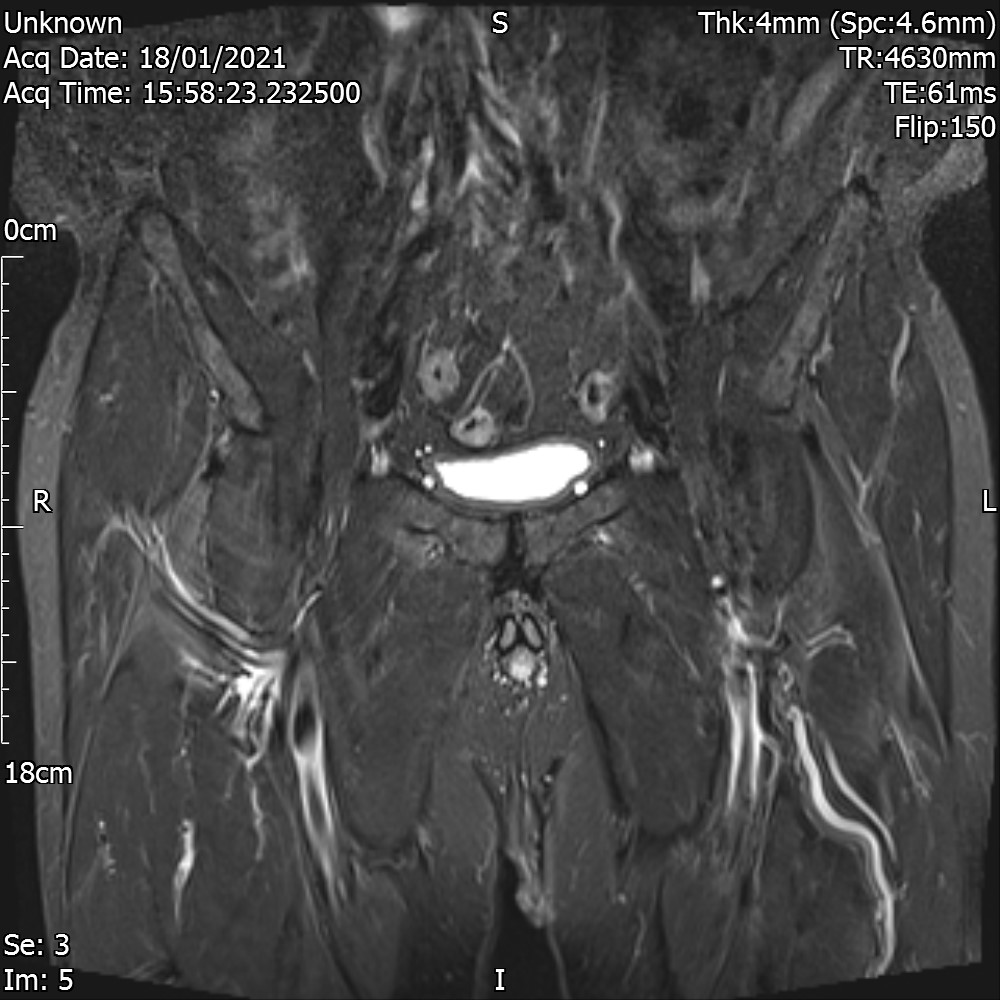




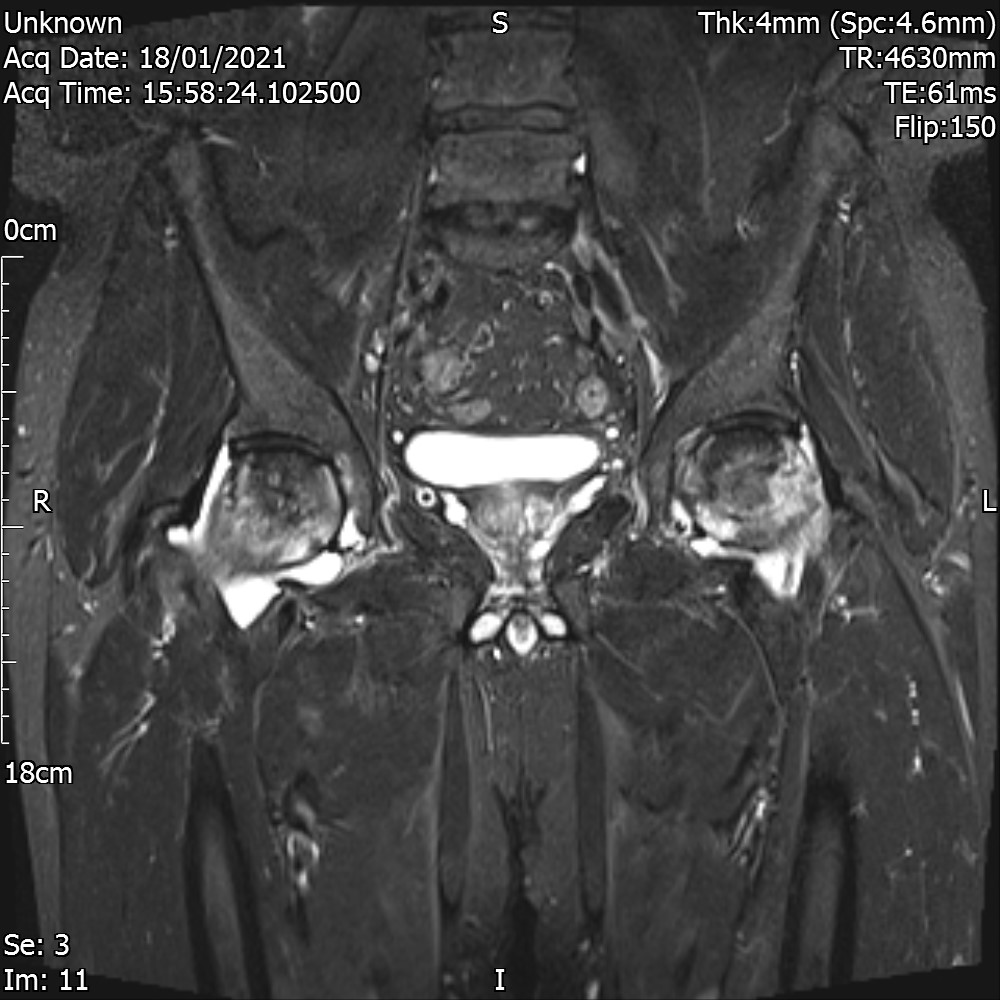













Coronal T1




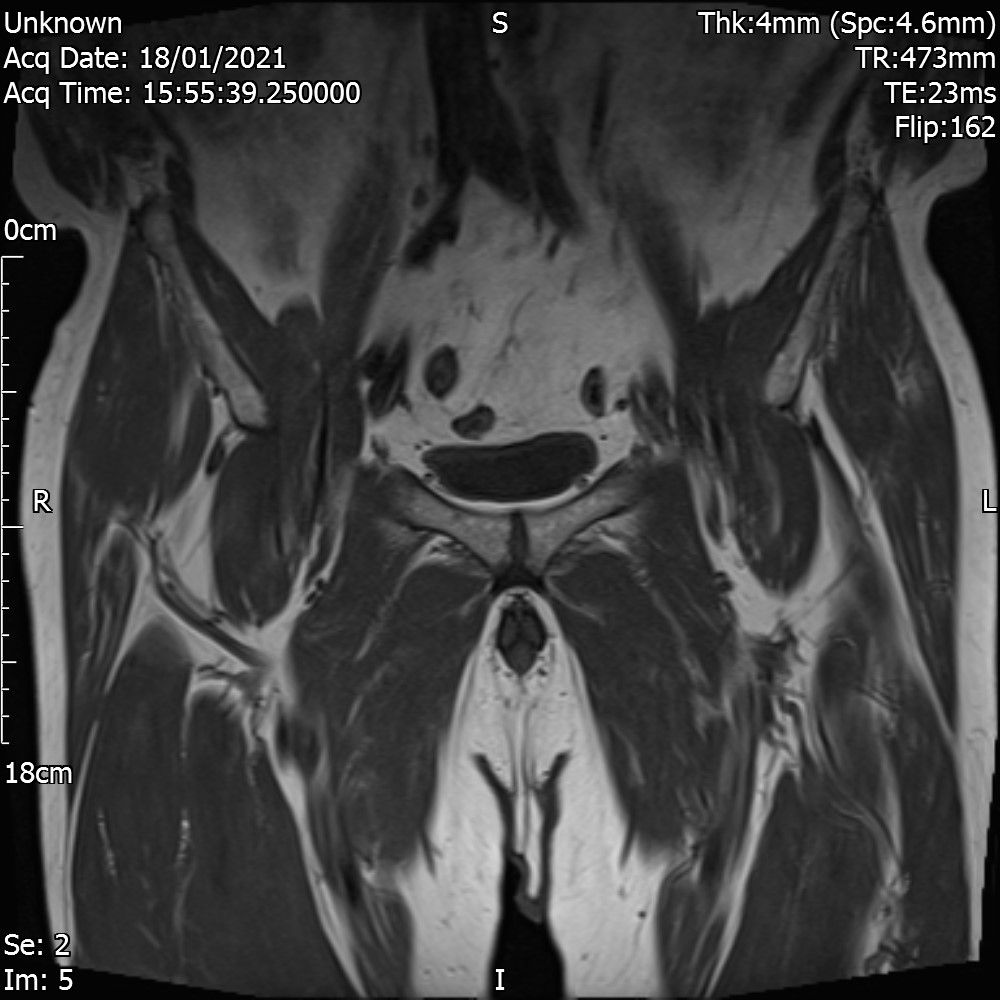


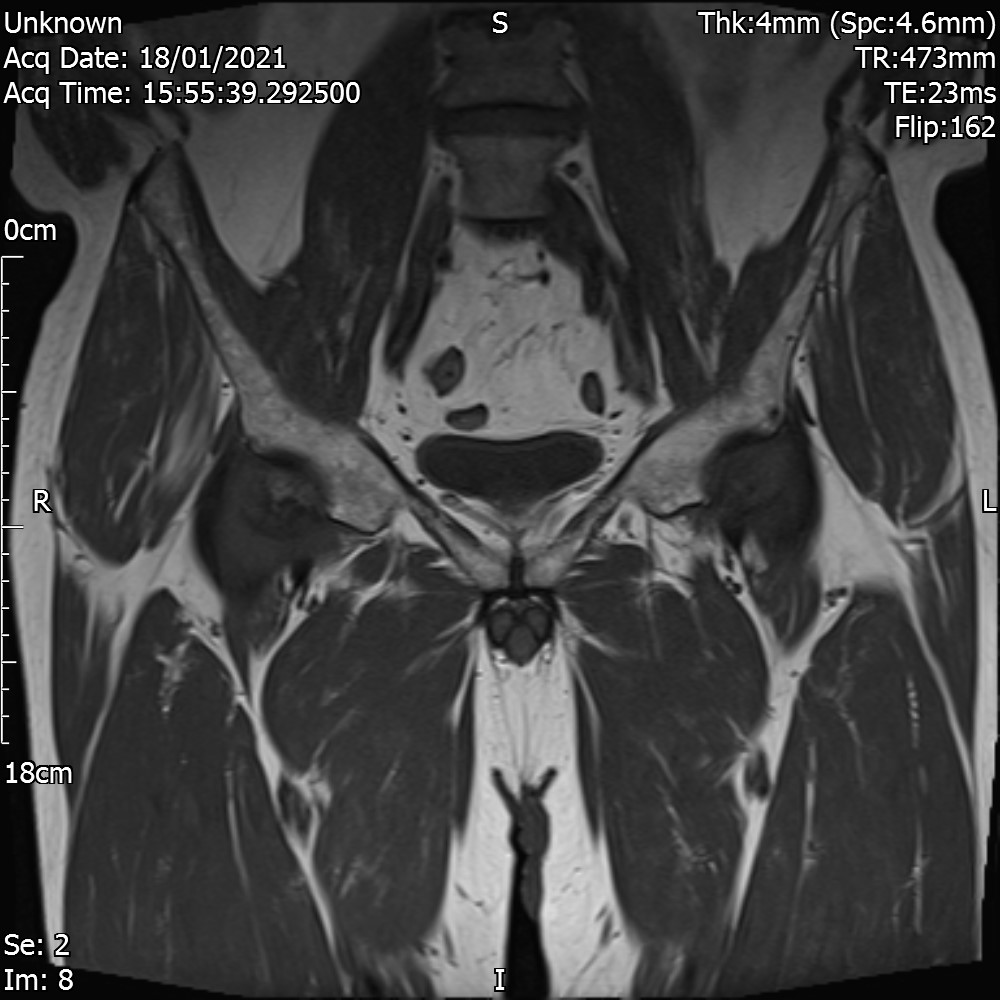

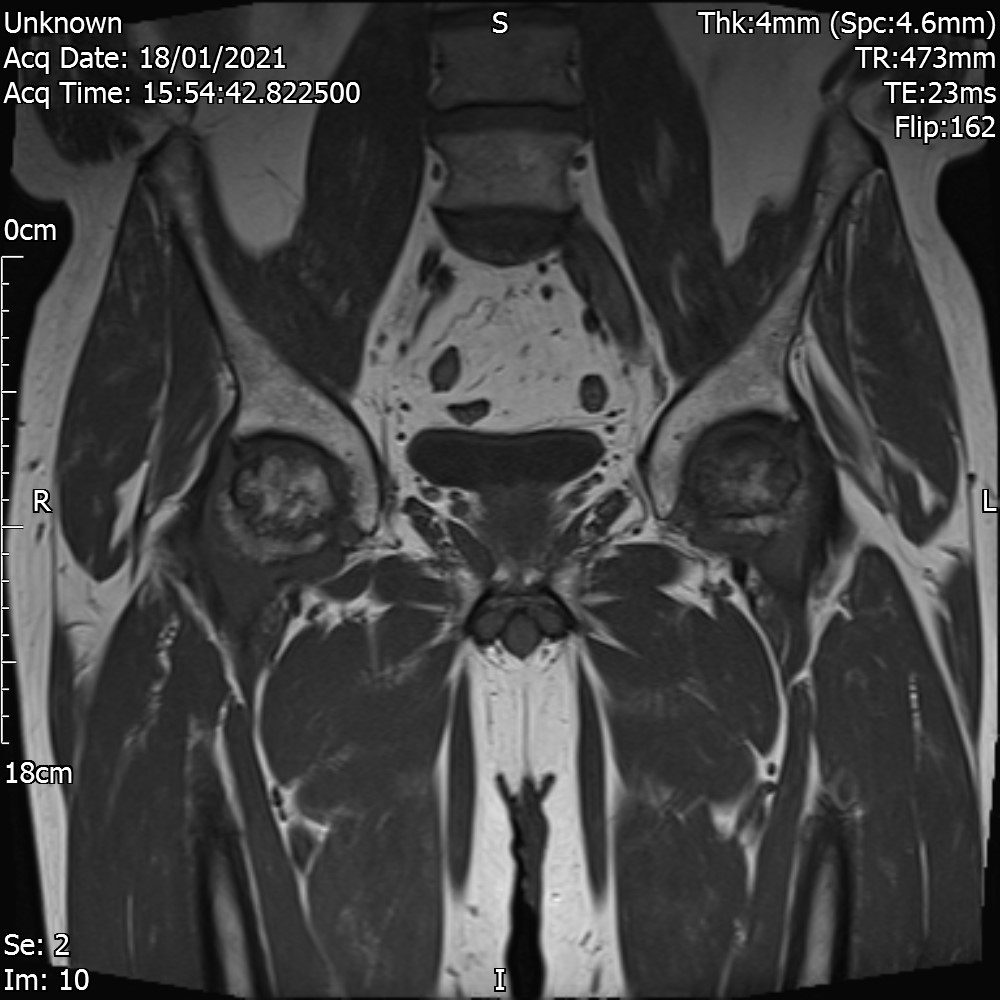














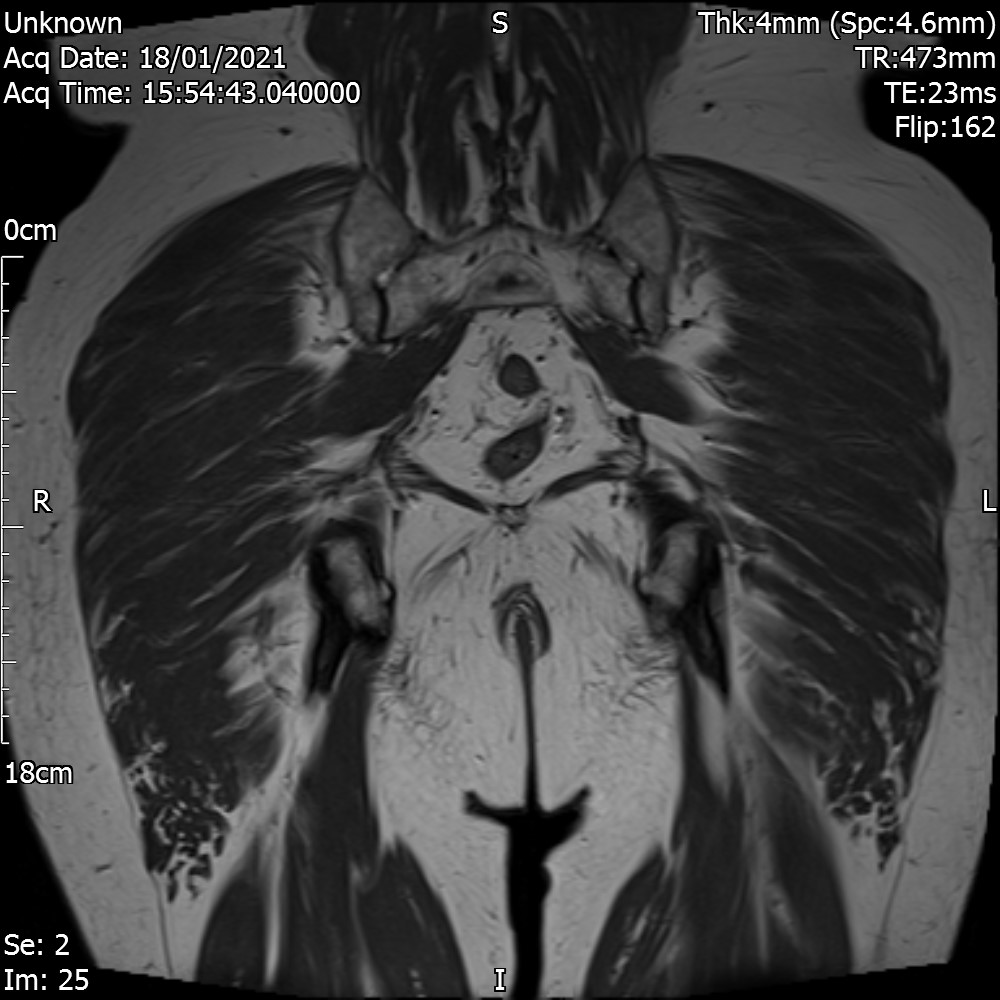





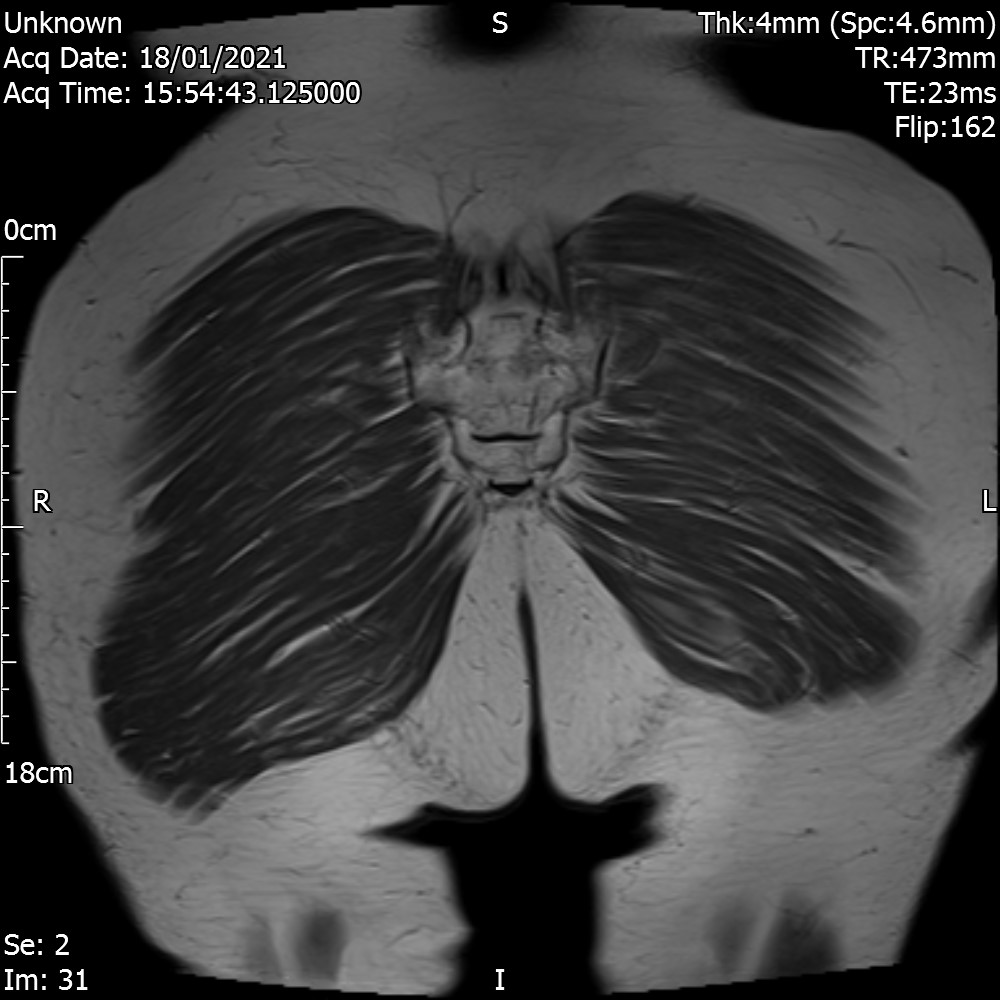

There is patchy oedema and sclerosis in both femoral heads and necks in keeping with osteonecrosis. There is some early fragmentation but there is no significant collapse.
There are bilateral effusions.
The marrow signal is otherwise within normal limits but there is an incidental lesion in the left posterior ilium. This shows slightly heterogeneous signal but there is a narrow zone of transition and a sclerotic margin. This may be an incidental chondroid lesion.
There is no significant tendinopathy or further soft tissue abnormality
CONCLUSION
Acute on chronic bilateral femoral head osteonecrosis grade 2/3 .
Orthopedic hip opinion is suggested
Analysis
There was nothing significant in the history to suggest any cause for the occurrence. A deeper look into the medical history revealed that the patient consumed 70 units of alcohol per week. However this data was last updated 6 years ago. No contemporary information was available about this.
Etiologic Factors Associated with Osteonecrosis
Traumatic-associated risk factors
- Femoral neck fracture
- Dislocation or fracture-dislocation
- Sickle cell disease
- Hemoglobinopathies
- Caisson disease (dysbarism)
- Gaucher disease
- Radiation
Atraumatic-associated risk factors
- Corticosteroid administration
- Alcohol use
- Systemic lupus erthyematosus
- Cushing disease
- Hypersecretion of cortisol (rare)
- Chronic renal failure/hemodialysis
- Pancreatitis
- Pregnancy
- Hyperlipidemia
- Organ transplantation
- Intravascular coagulation
- Thrombophlebitis
- Cigarette smoking
- Hyperuricemia/gout
- HIV
- Other potential risk factors
- Idiopathic causes
Ref: Osteonecrosis of the Hip: A Primer
Glucocorticoid-induced Osteonecrosis develops in 9% to 40% of patients receiving long-term therapy, and develops much less frequently in patients receiving short-term therapy.
Osteonecrosis due to alcoholism is believed to result from decreased bone genesis caused by excess lipid formation and increased intracellular lipid deposits, leading to osteocyte death.
High doses of corticosteroids and excessive alcohol use together present the highest associated direct risk factors for the development of hip ON and account for more than 80% of cases not related to trauma.
Treatment Options
Restricting weight-bearing with the use of assistive devices such as crutches or a cane may be useful to control symptoms of pain, weakness, and antalgic gait.
NSAIDs may provide temporary pain relief.
Surgical options
Core decompression – The procedure involves drilling holes into the femoral head to relieve pressure and create channels for new blood vessels to nourish the affected areas. The published success rates of core decompression vary greatly from 40% to 100%, depending on patient population. Higher success rates are seen in early stage.
- Bone Grafting
- Bone Marrow Aspirate Concentration
- Percutaneous Drilling
- Vascularised Bone Graft
- Total Hip Arthroplasty
- Bisphosphonate Therapy - A Paradigm Shift in Osteonecrosis Treatment with Bisphosphonates