Bony Mets – No Primary | Cases
Published on Jan 6, 2021
Skeletal Metastases of Unknown Primary – SMUP
Presentation
- 64 male, Retired, likes walking.
- C/o: Right sided lumbosacral pain. No reported P+N or Numbness.
- Onset – 6 weeks, insidious. Ongoing left knee issue. Patient reports the onset of back pain was gradual. He linked it to the knee pain due to compensatory gait.
- Pain worse with sustained sitting, standing, bending.
- Reports nothing helps the pain.
- Pain worse at end of the day. No change in morning. Information about sleep not available.
- Weight loss – 1.5 stones over 3 months. Patient also reports lack of appetite. Links weight loss to lack of appetite. Reports that the weight has stabilised now.
- No bladder / bowel issues, no saddle anaesthesia, no pain with cough sneeze, no trauma, no reported leg weakness, no bilateral pins and needles.
- Taking Naproxen.
- Expectation: diagnosis, pain relief
Examination
- Pain prevented most of the assessment.
- Minimal motor weakness in left foot PF and DF (grade 4-/5).
- Brisk knee and ankle jerks.
- Babinski reported as NAD. (clonus not mentioned)
- Reduced lumbar spine ROM – all movements.
Assessment
- Too painful to examine fully.
- No history of cancer (no primary).
- Clinician requested MRI lumbar and thoracic spine to rule out any sinister pathology.
MRI
Thoracic Spine - Sagittal T2 View
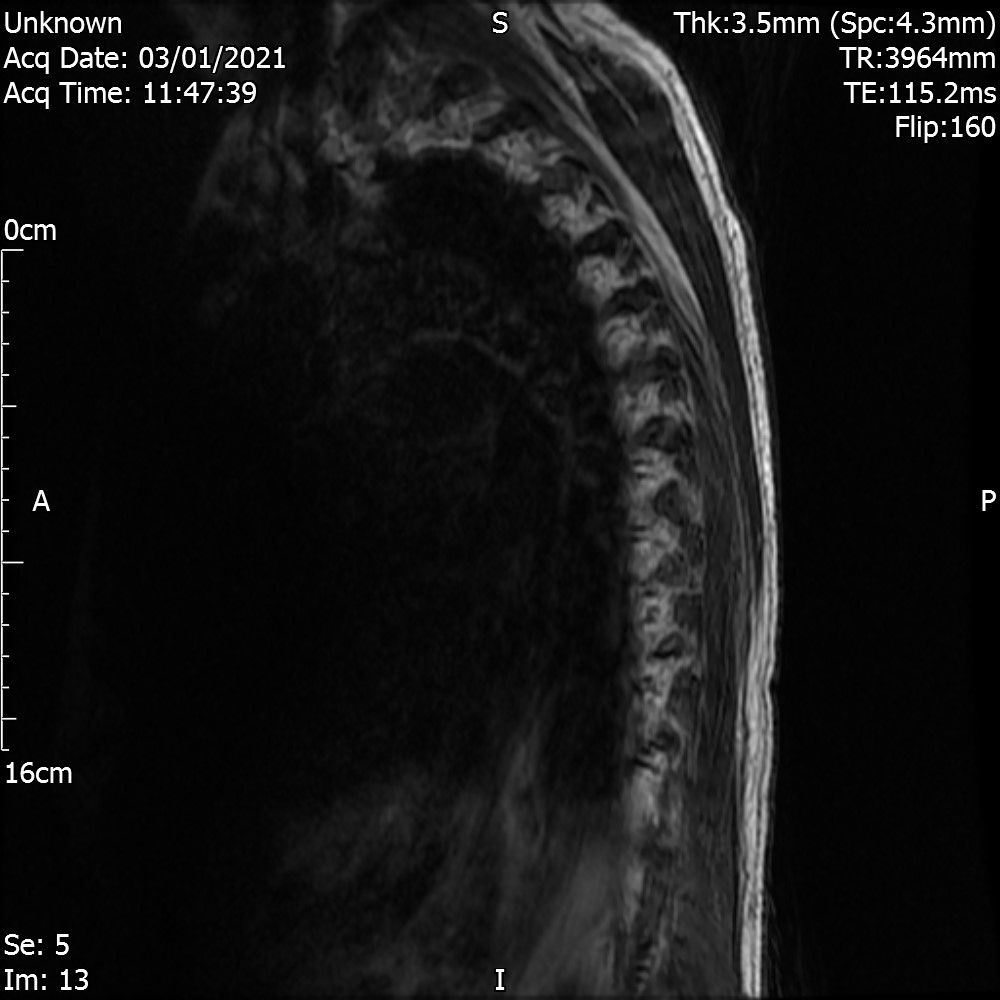
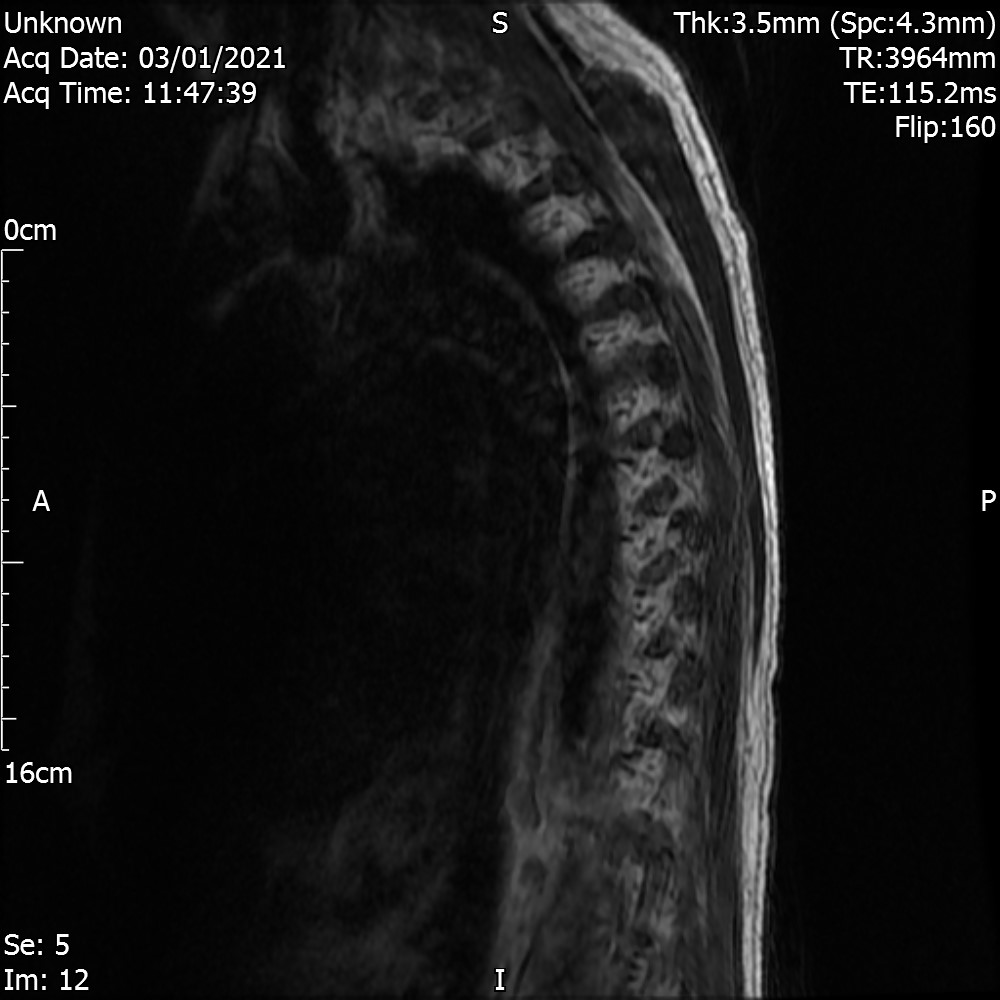
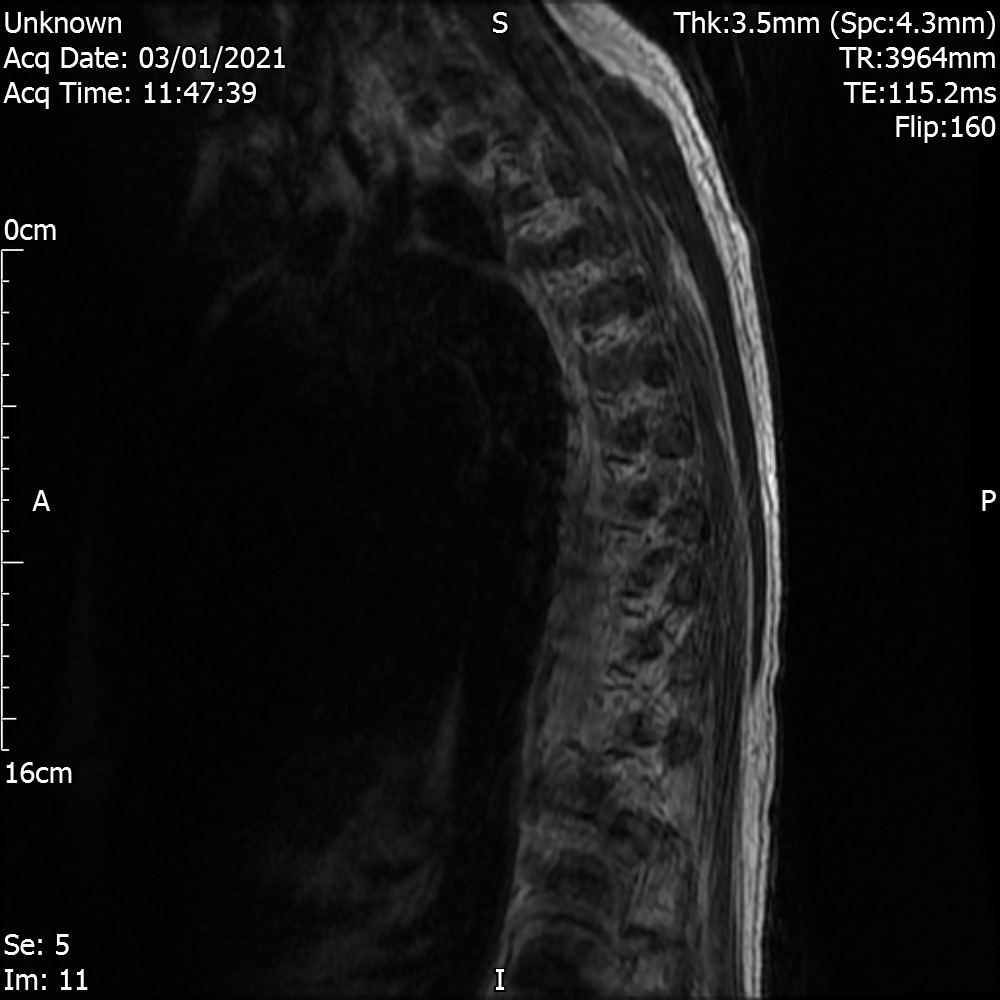
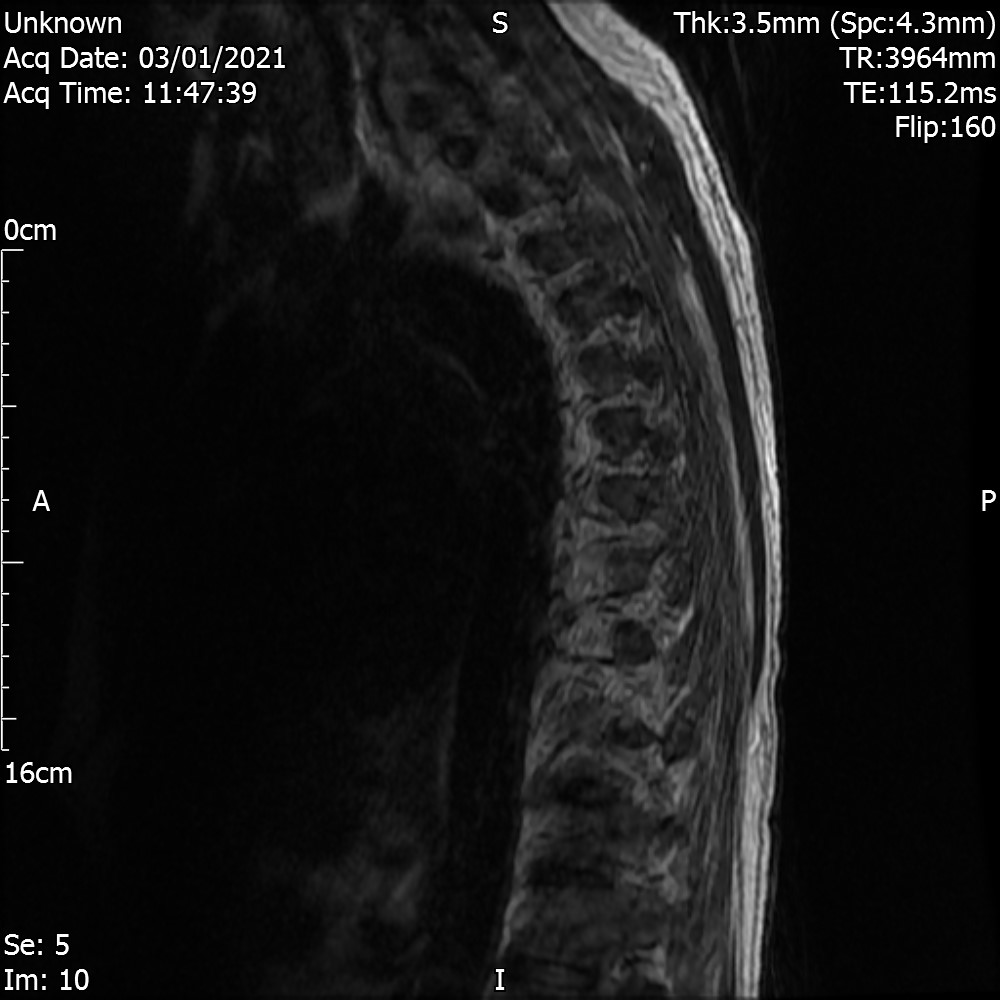
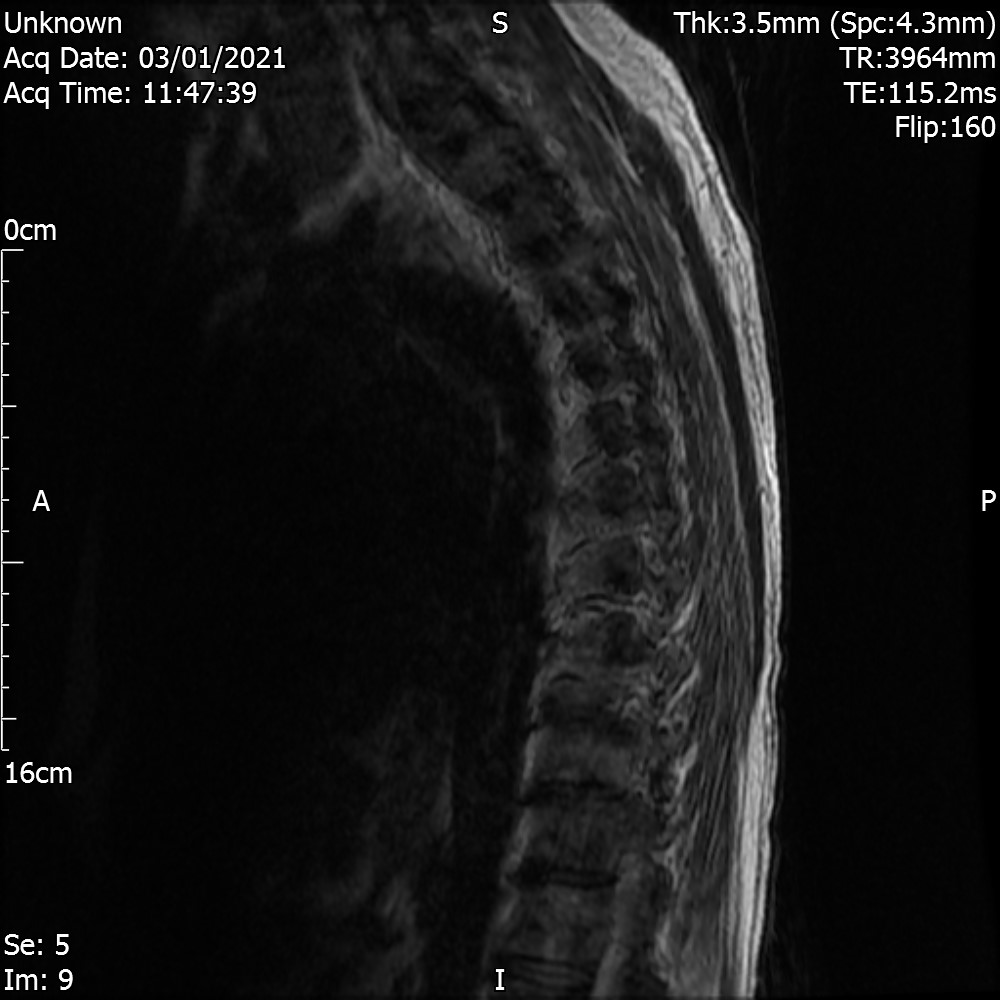
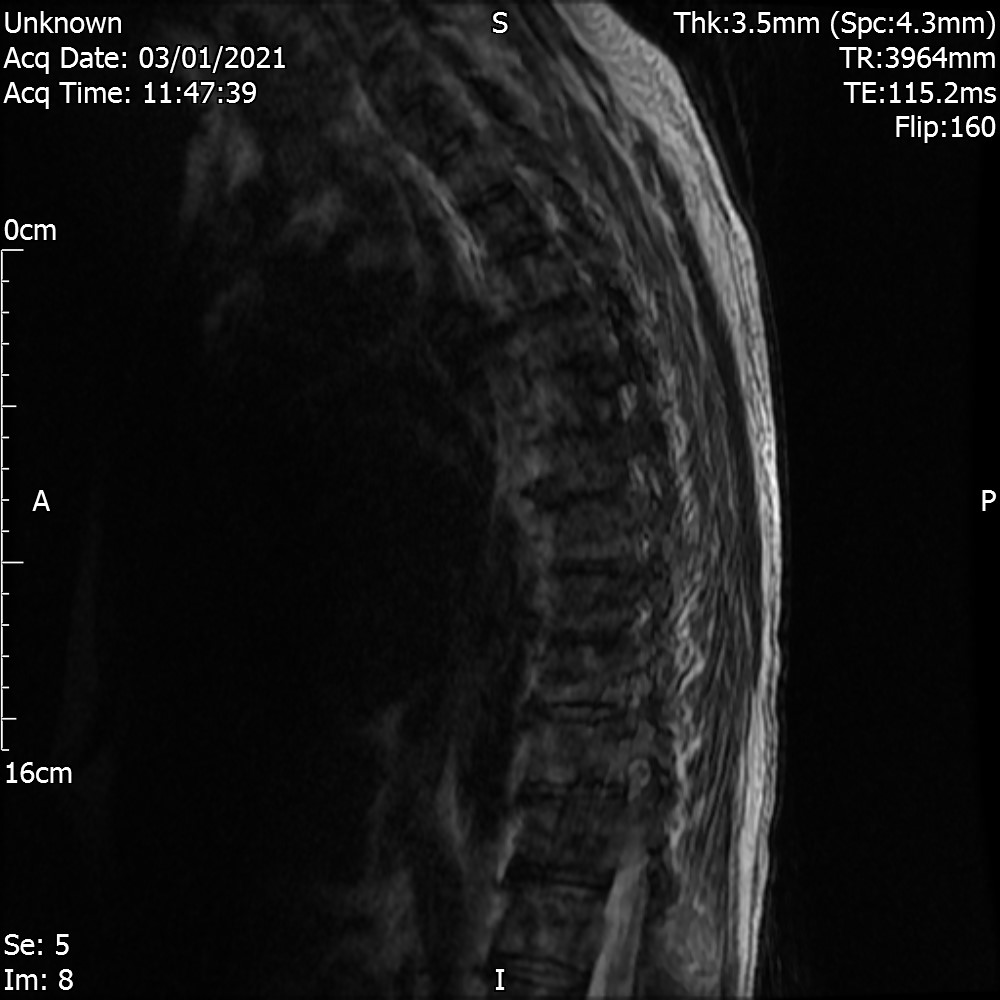
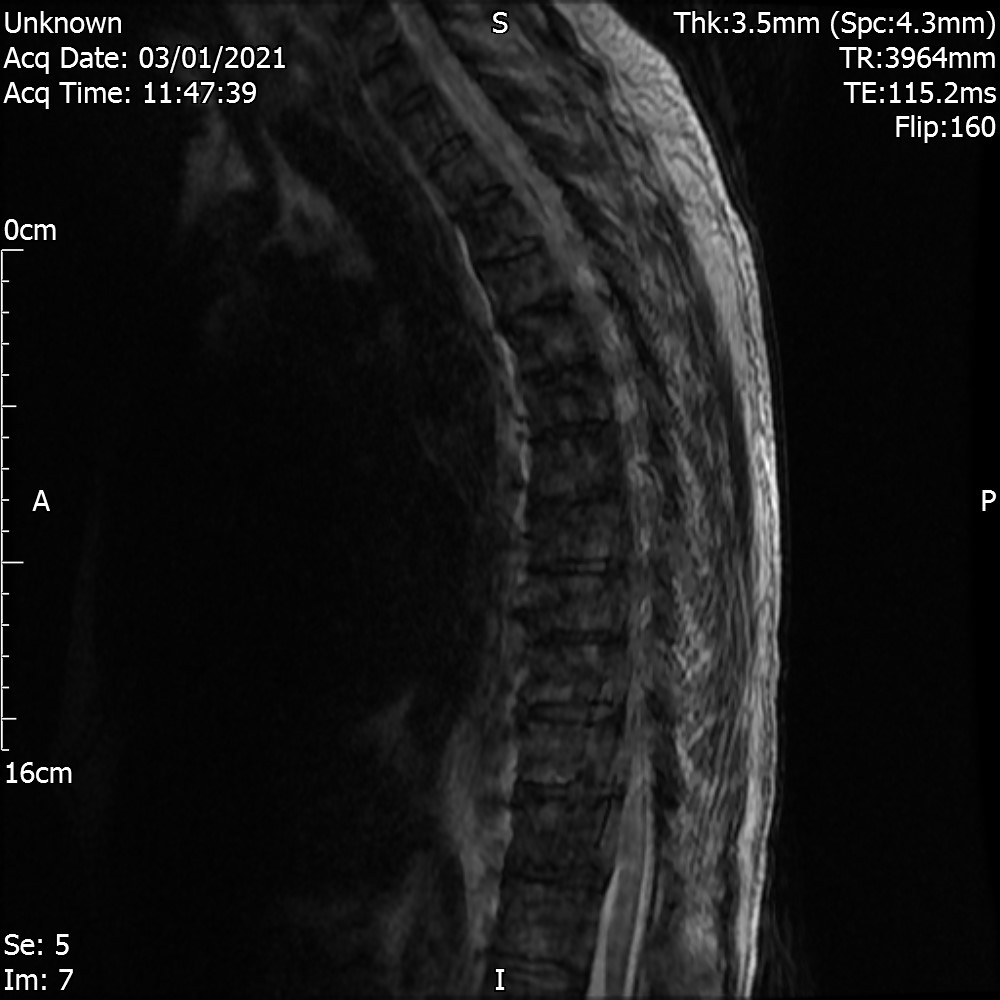
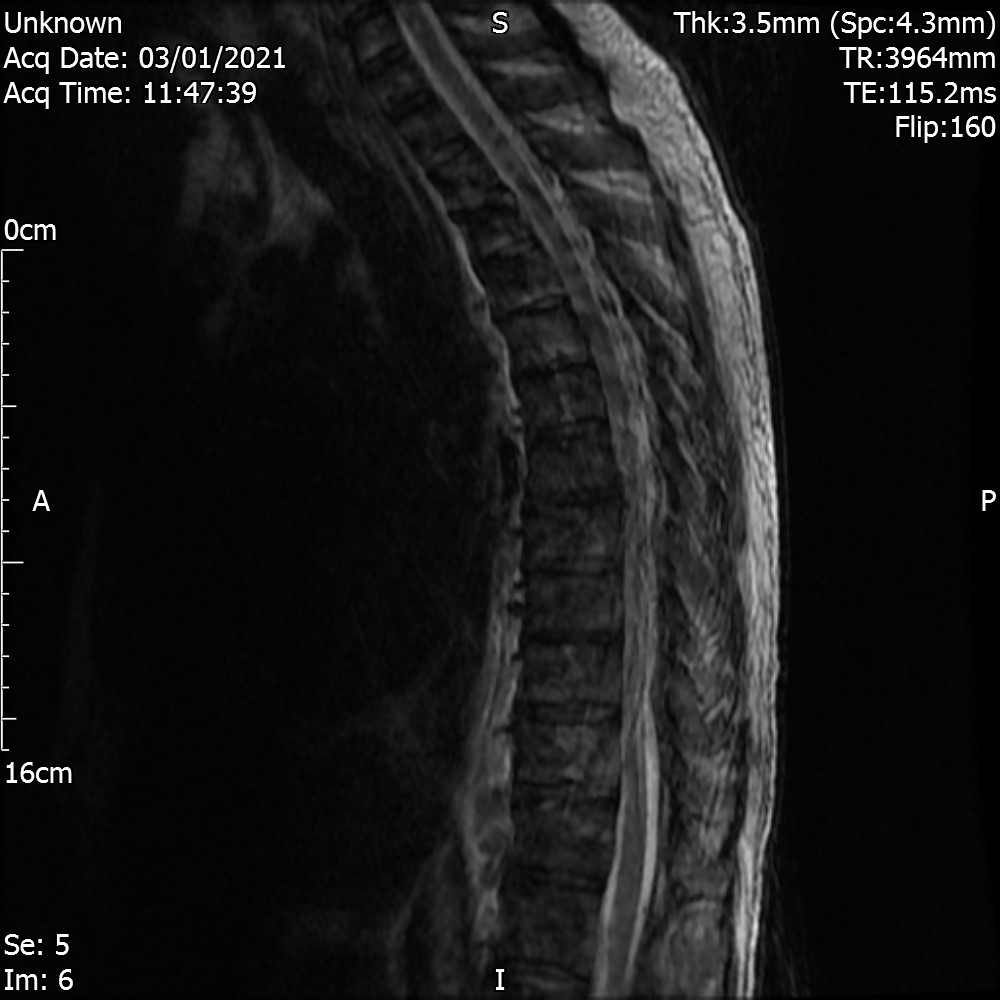
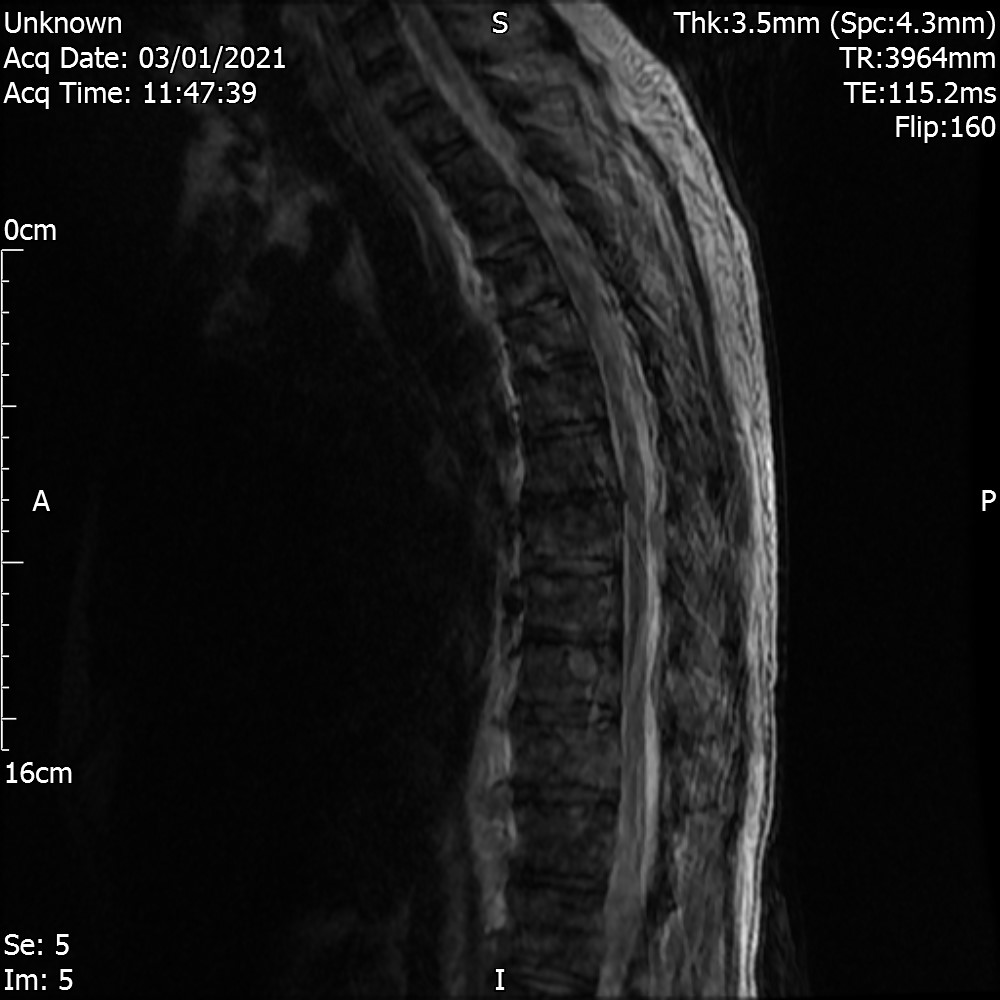
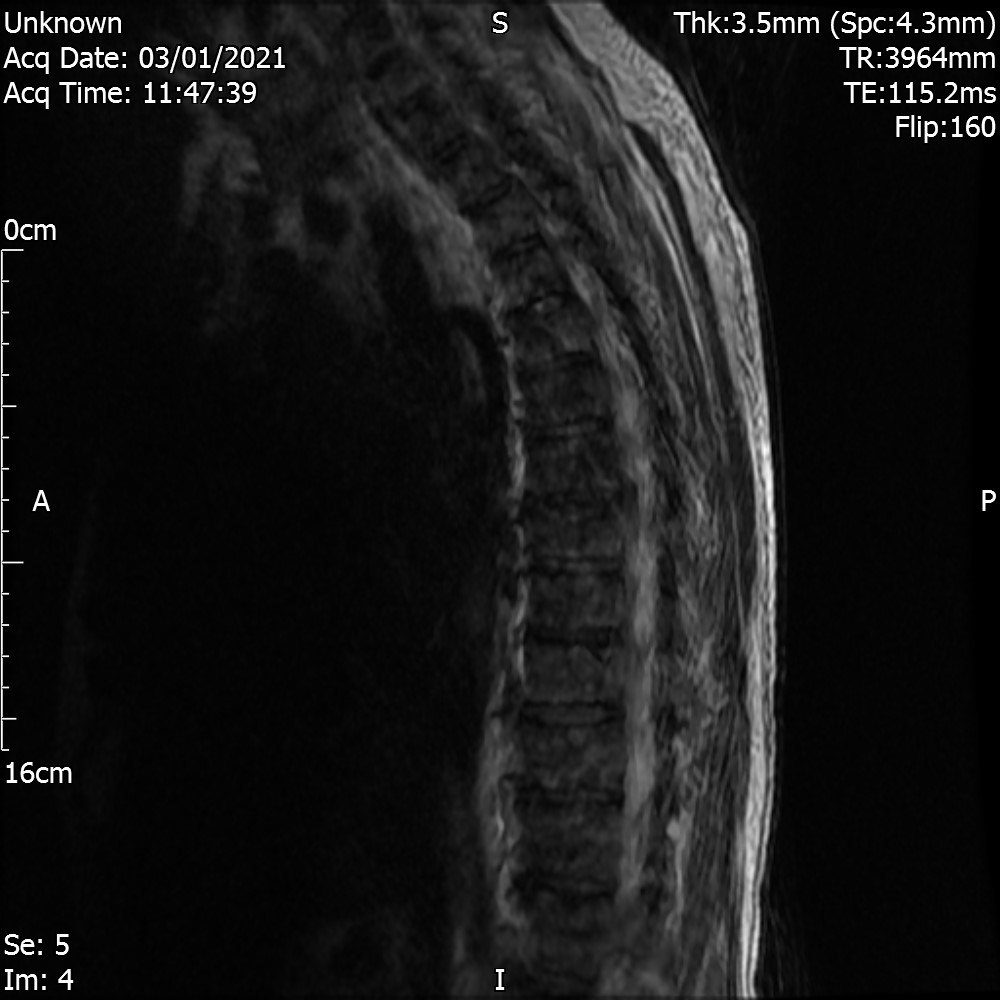
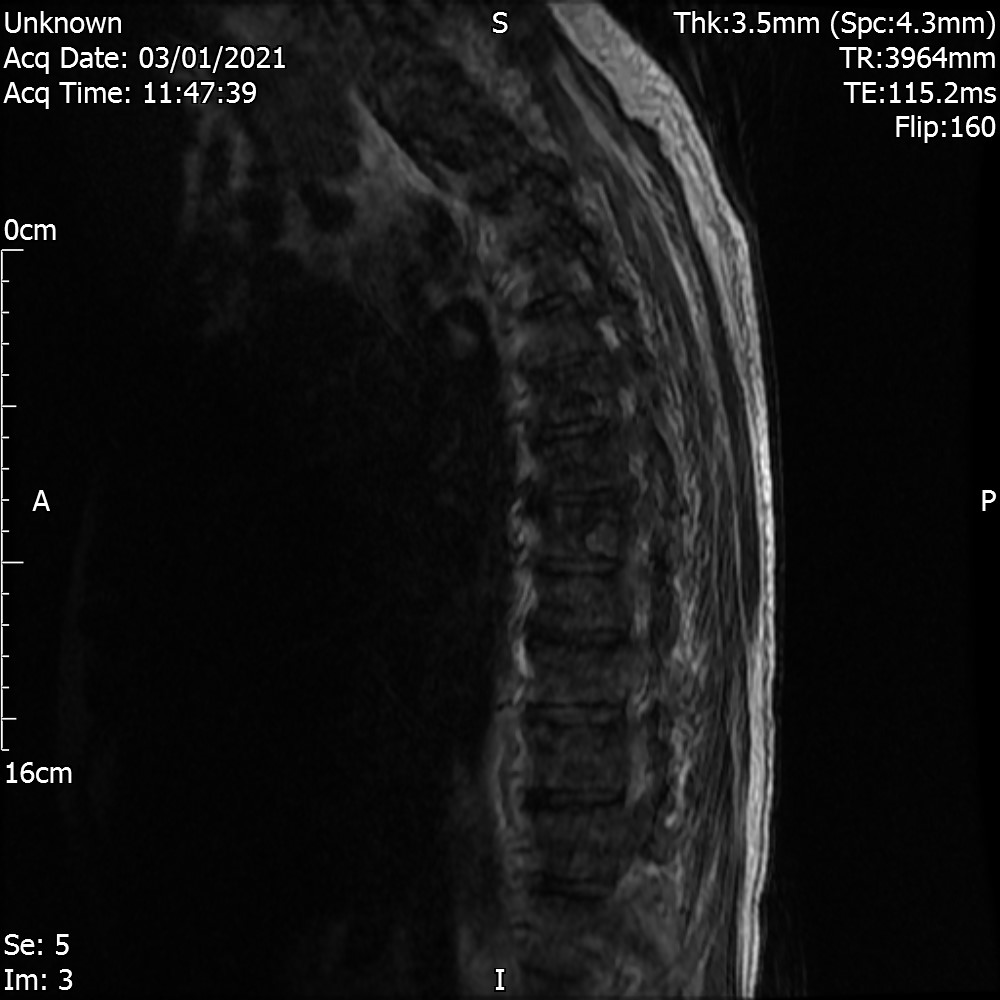
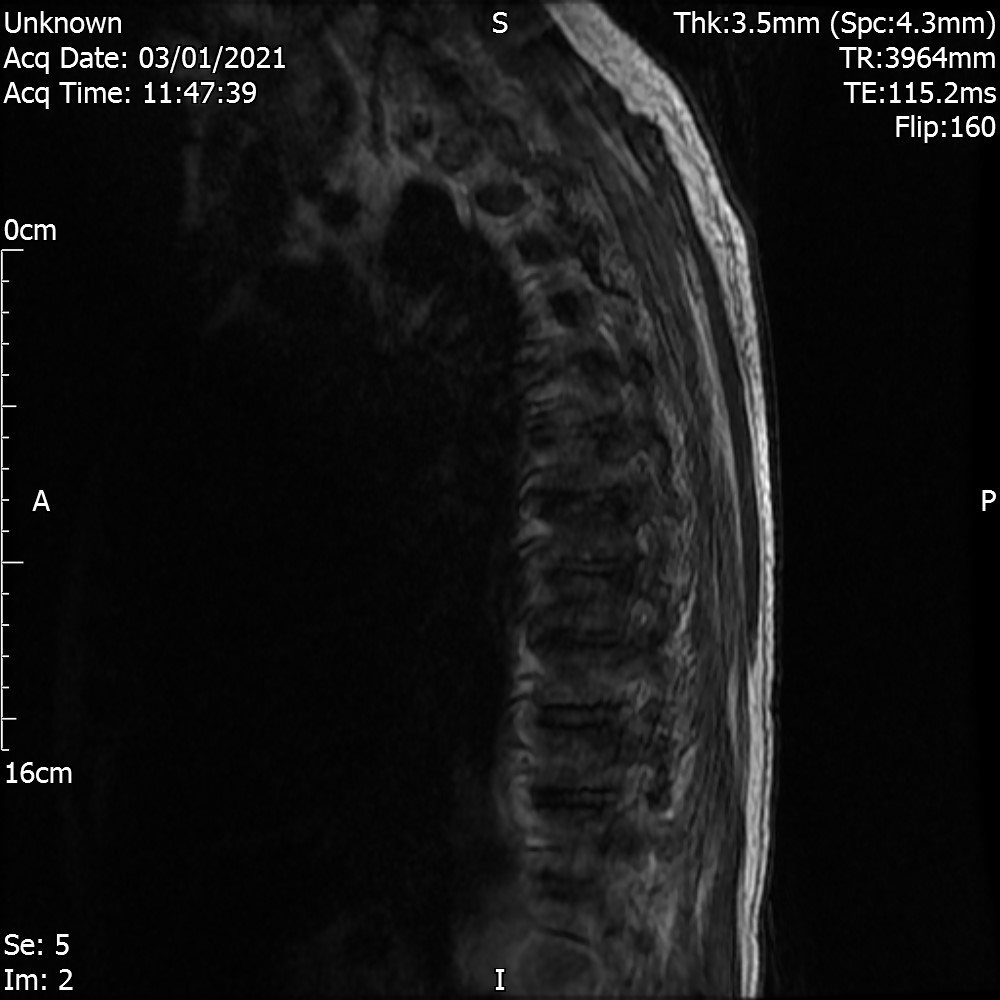
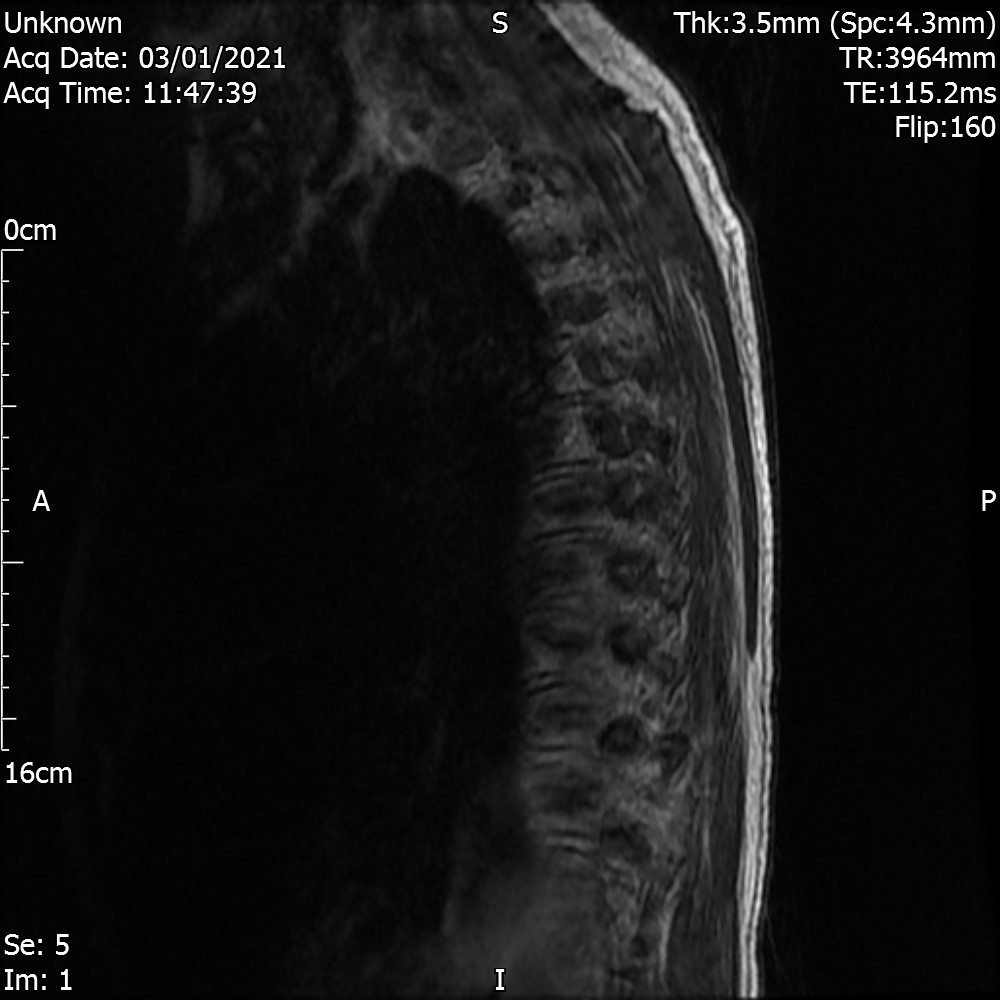
The central canal and visualised thoracic cord are clear but the study reveals extensive abnormality of the anterior column with focal replacement of T1 marrow signal consistent with small volume but diffuse metastatic bone disease. There is no evidence of vertebral collapse, fracture or active or imminent threat to the spinal canal There is movement artefact but is also likely that these changes involve the posterior elements. No intrinsic lesion or expansion of the cord seen.
CONCLUSION
Diffuse metastatic bone disease of the visualised skeleton. No intrinsic cord lesion or compression to explain symptoms.
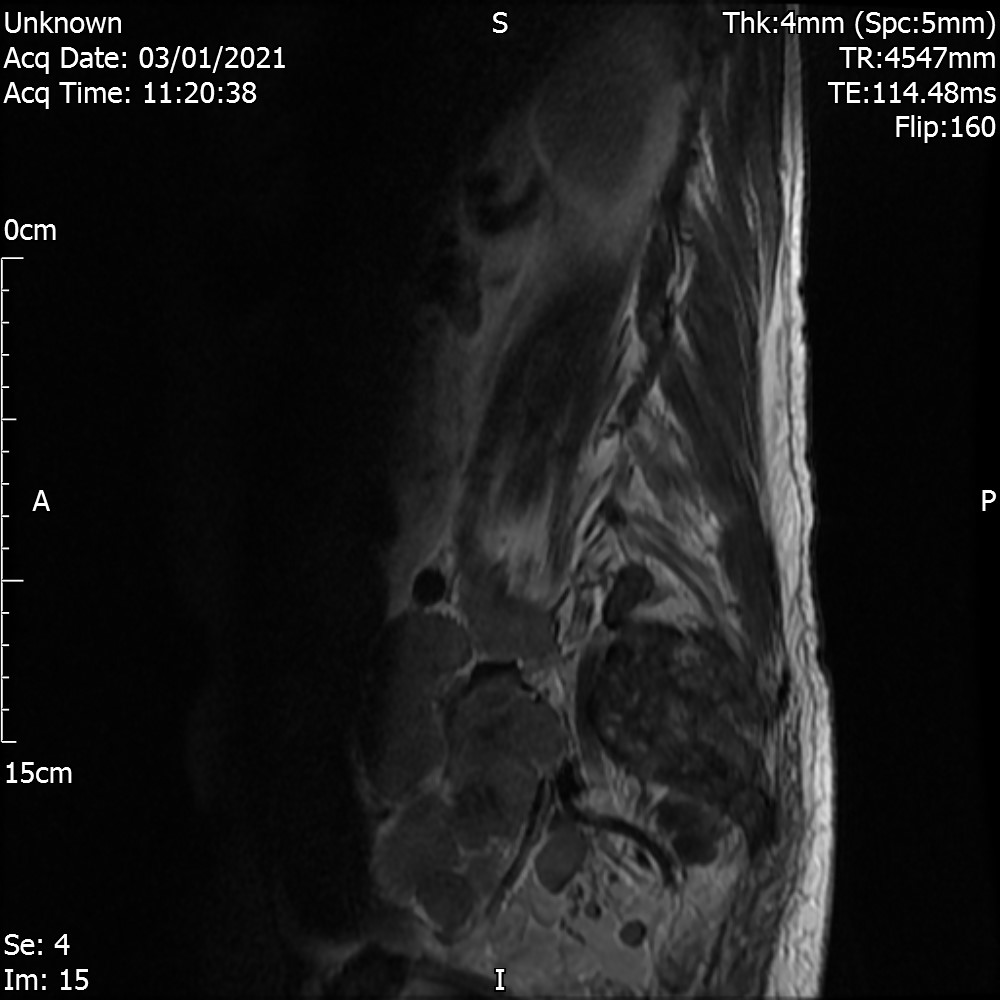
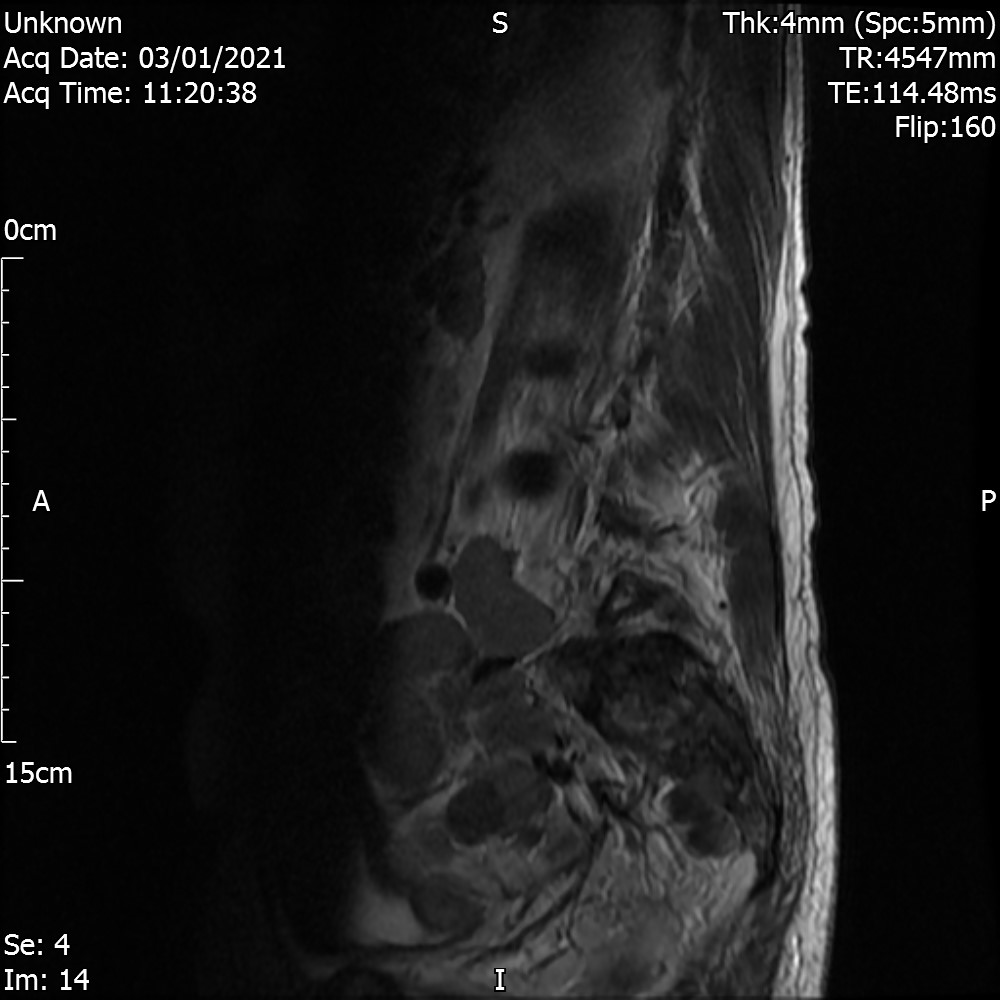
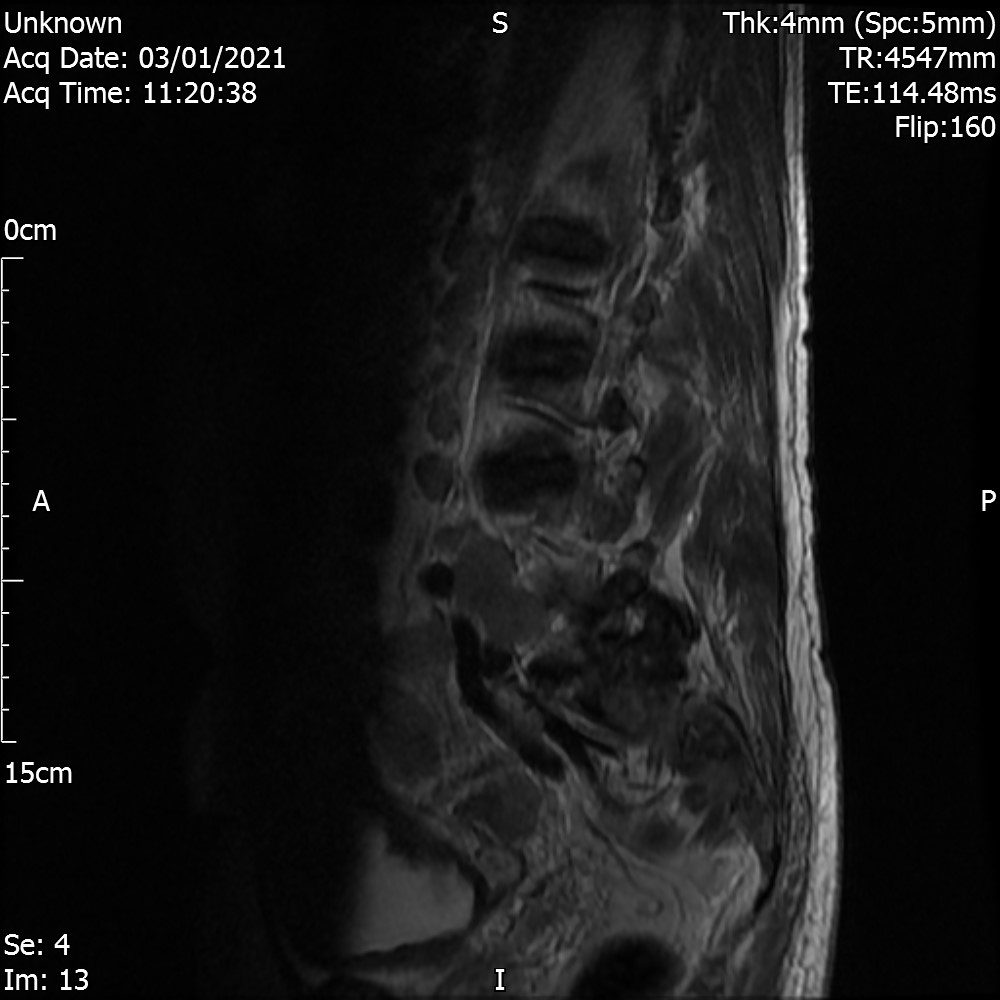
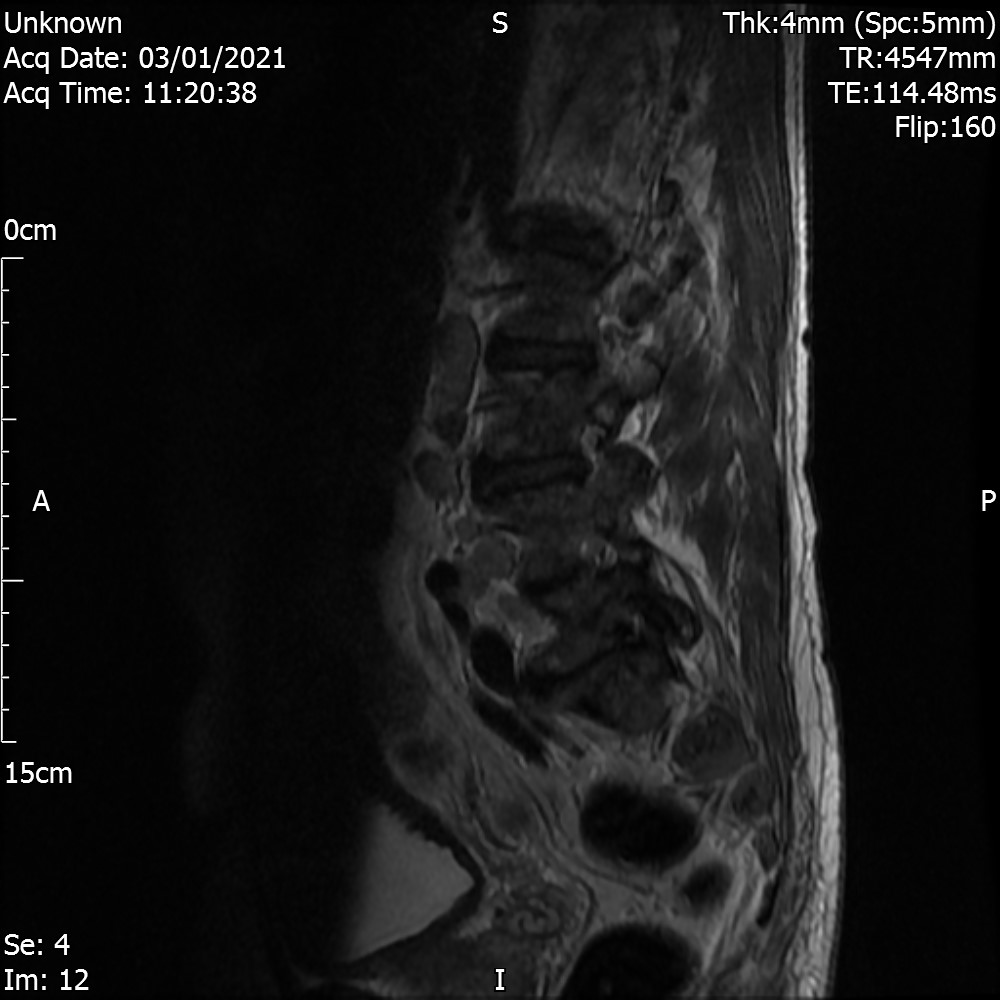
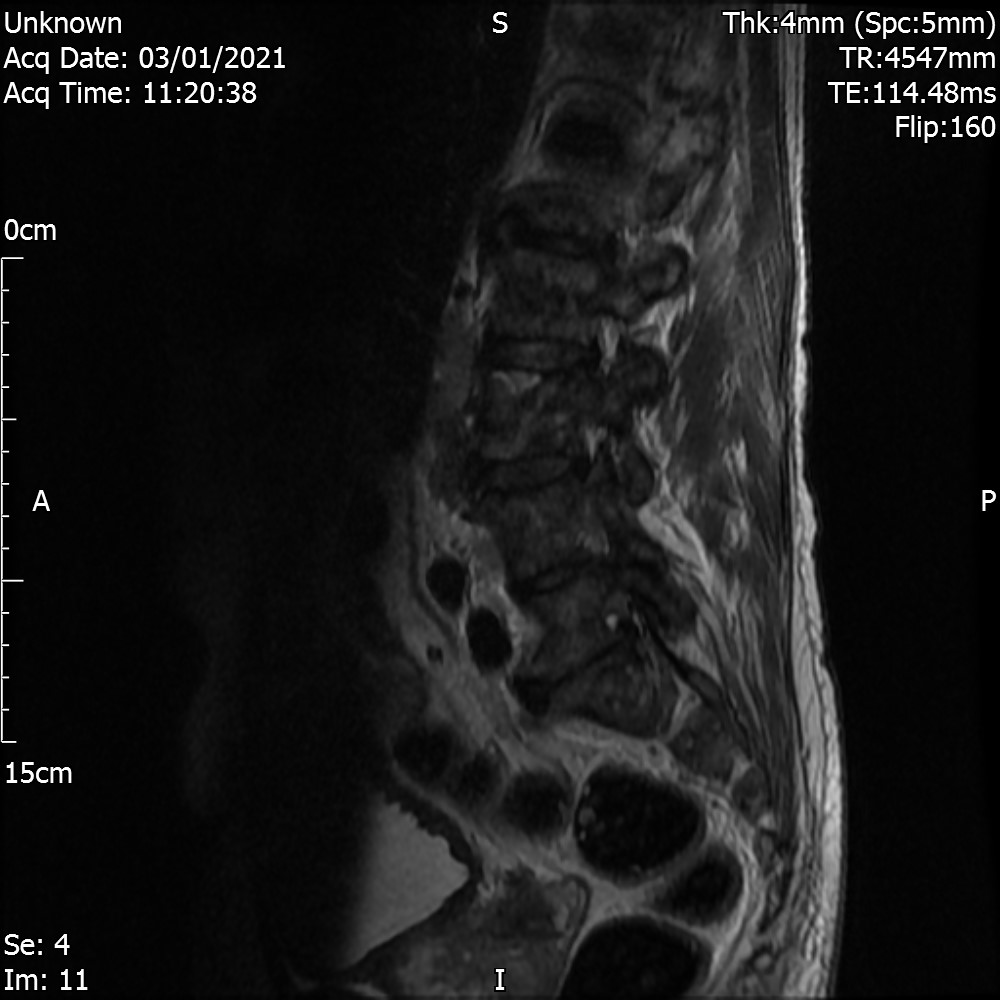
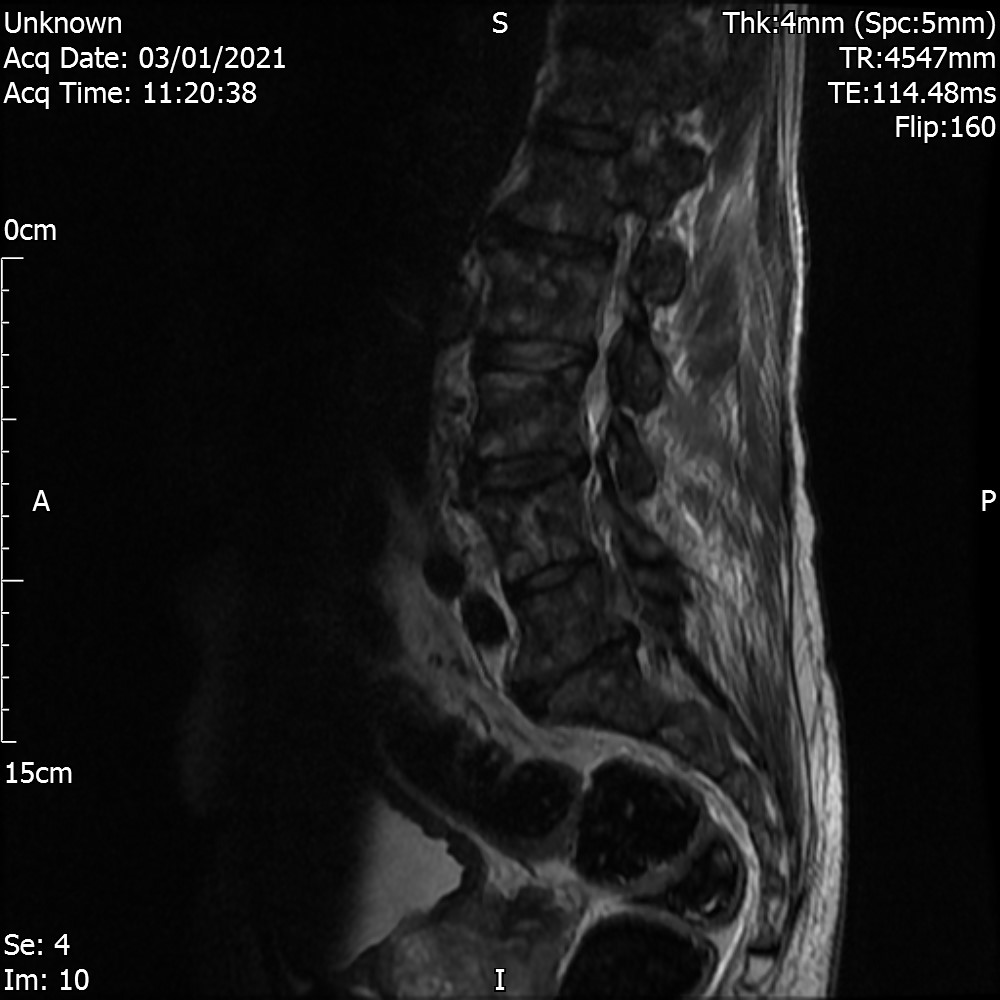
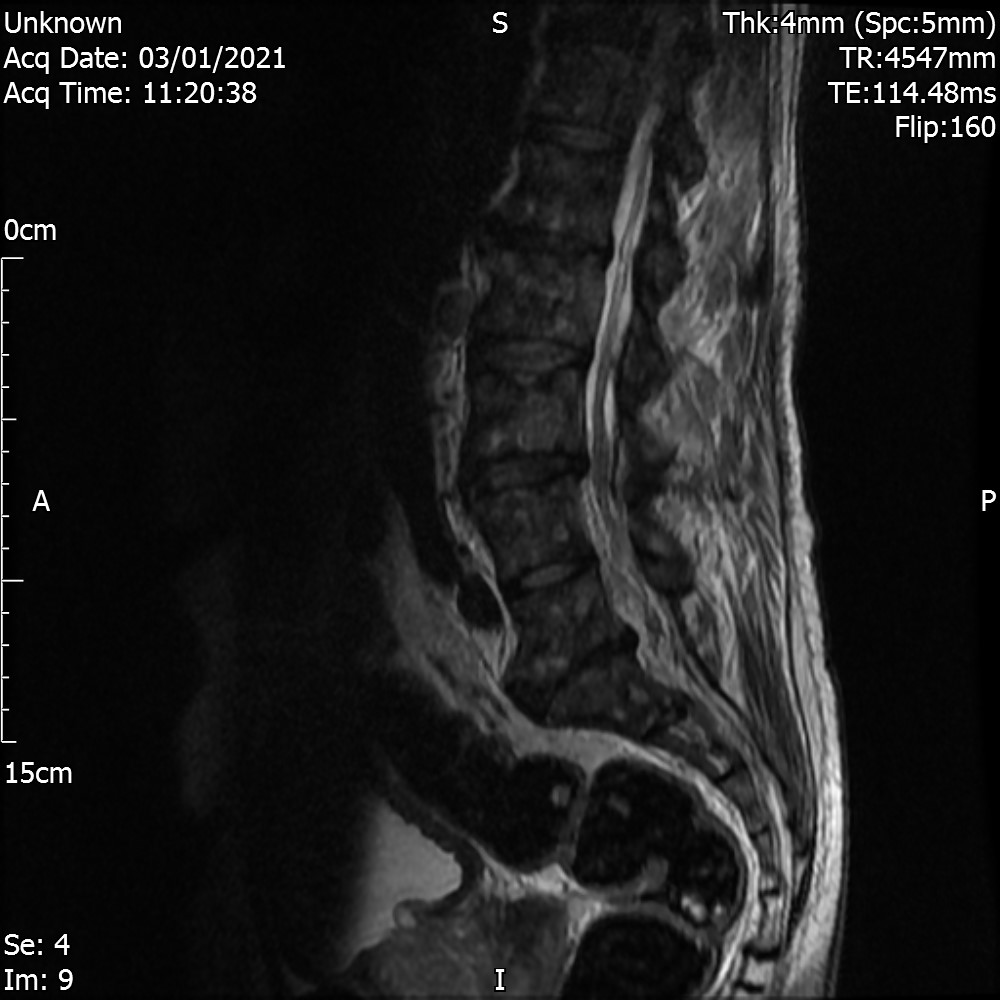
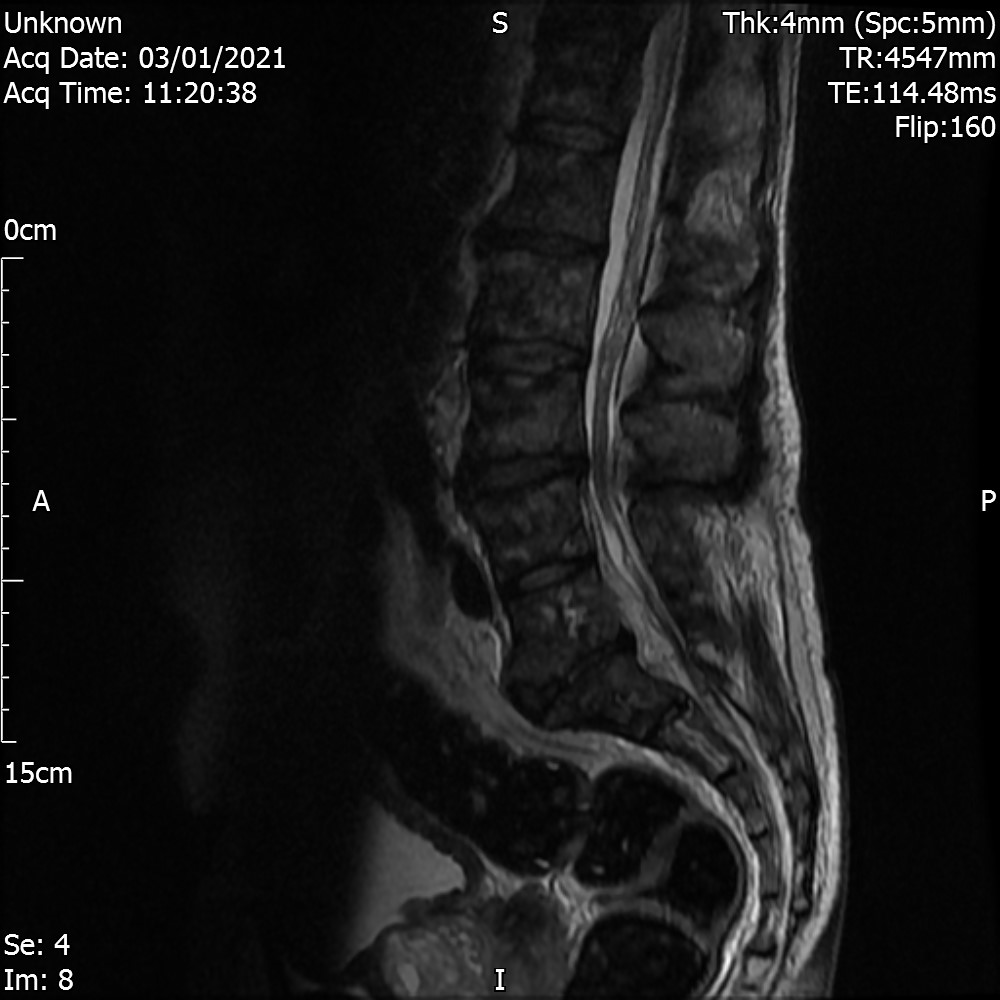
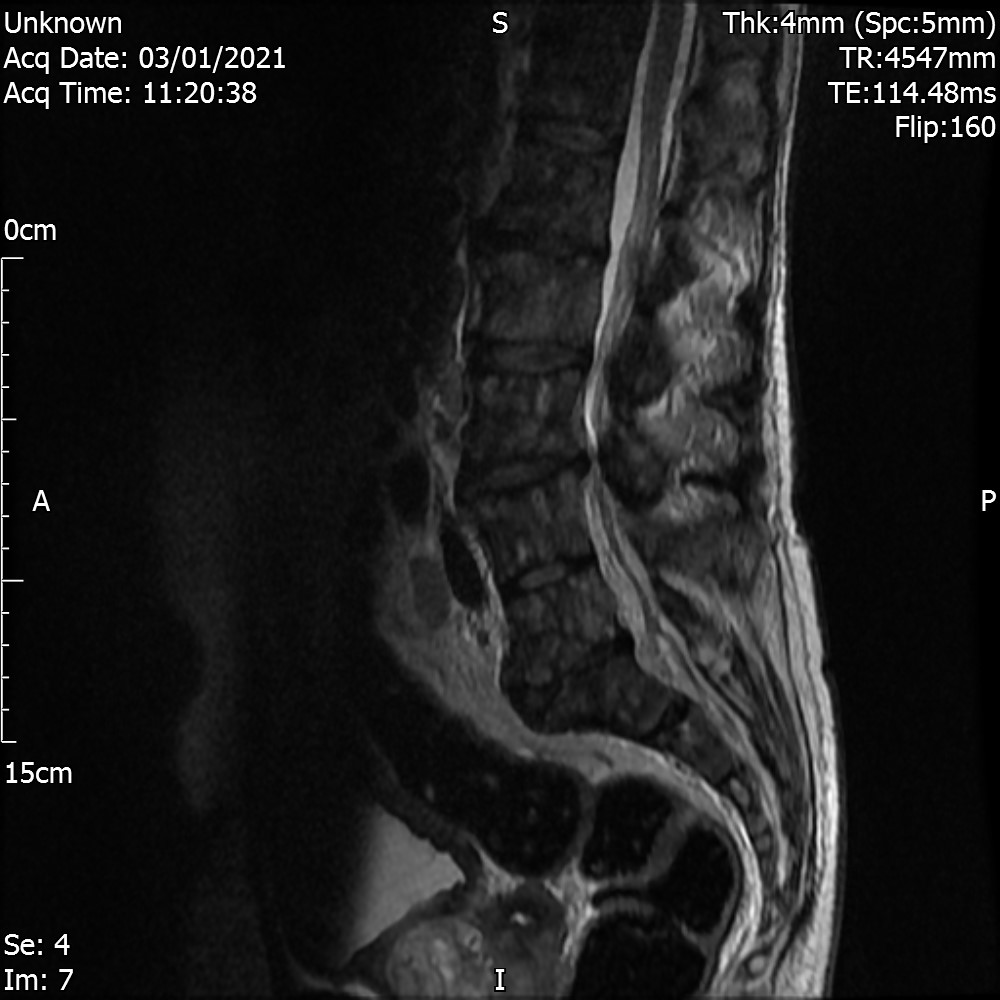
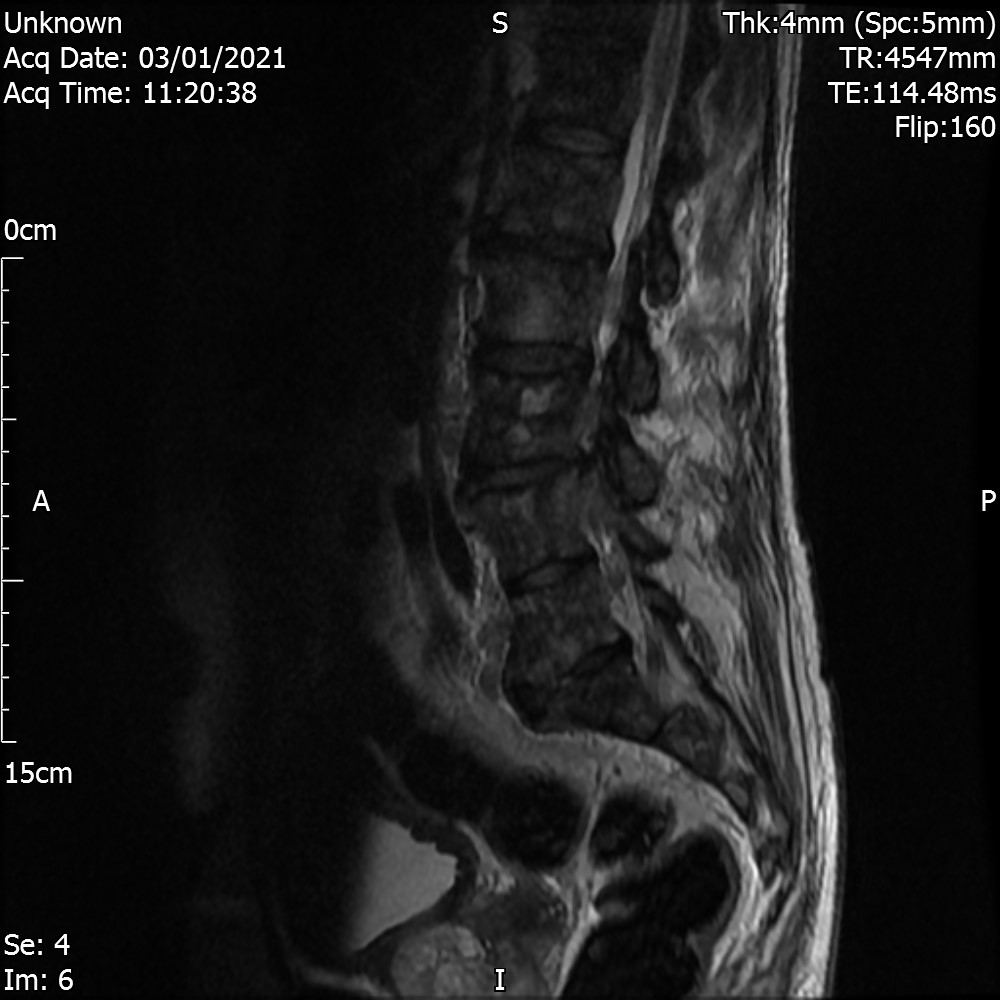
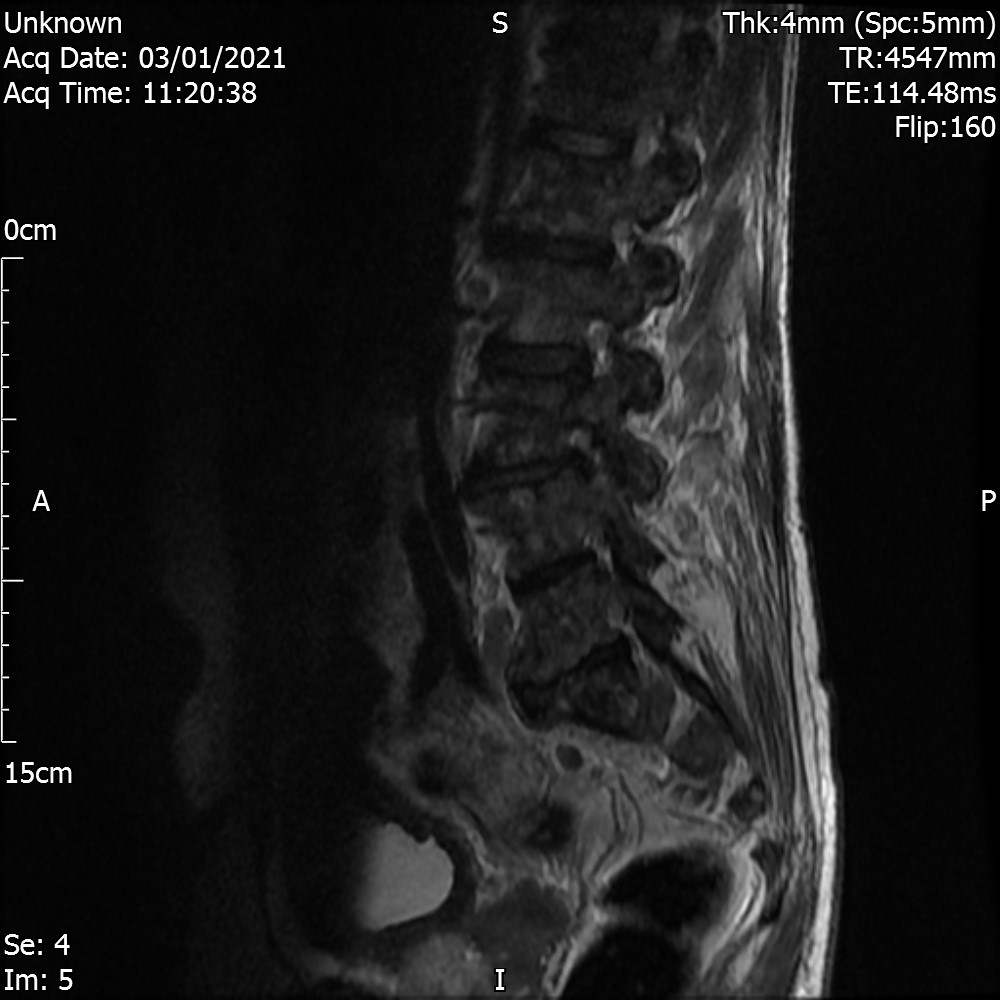
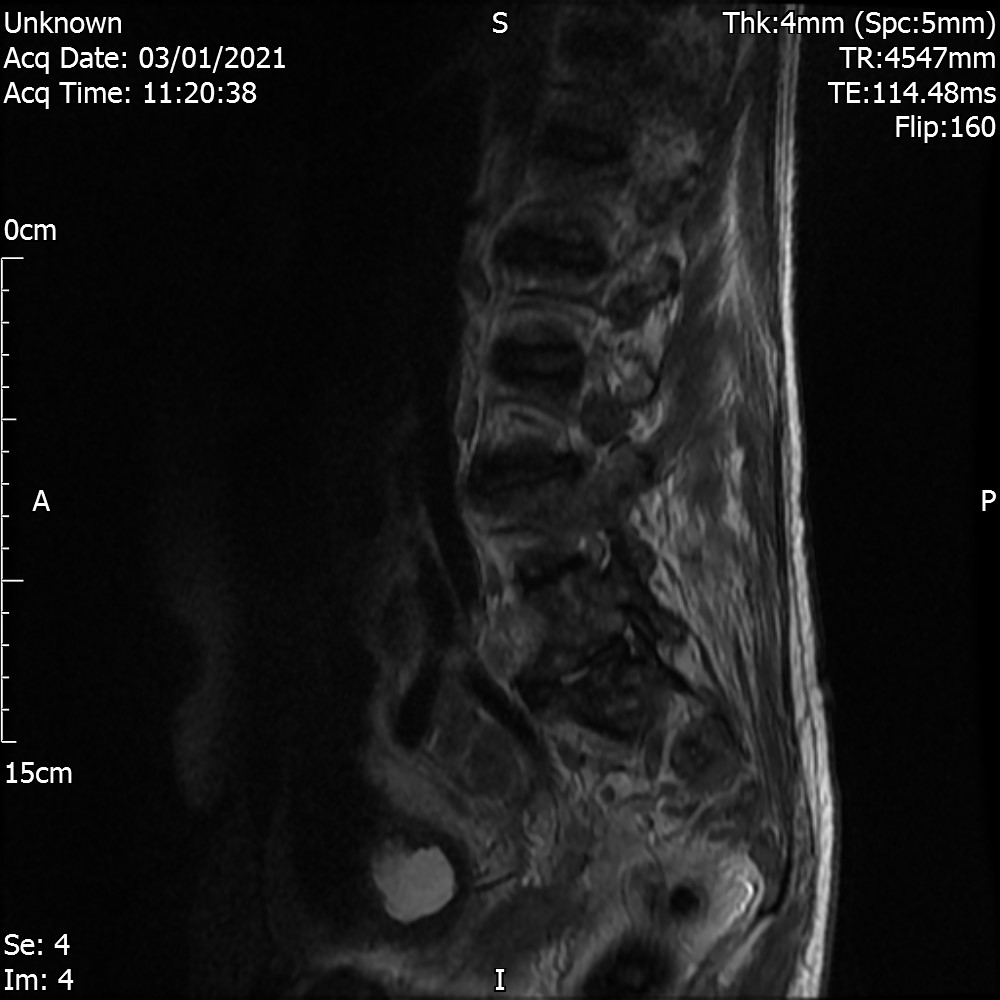
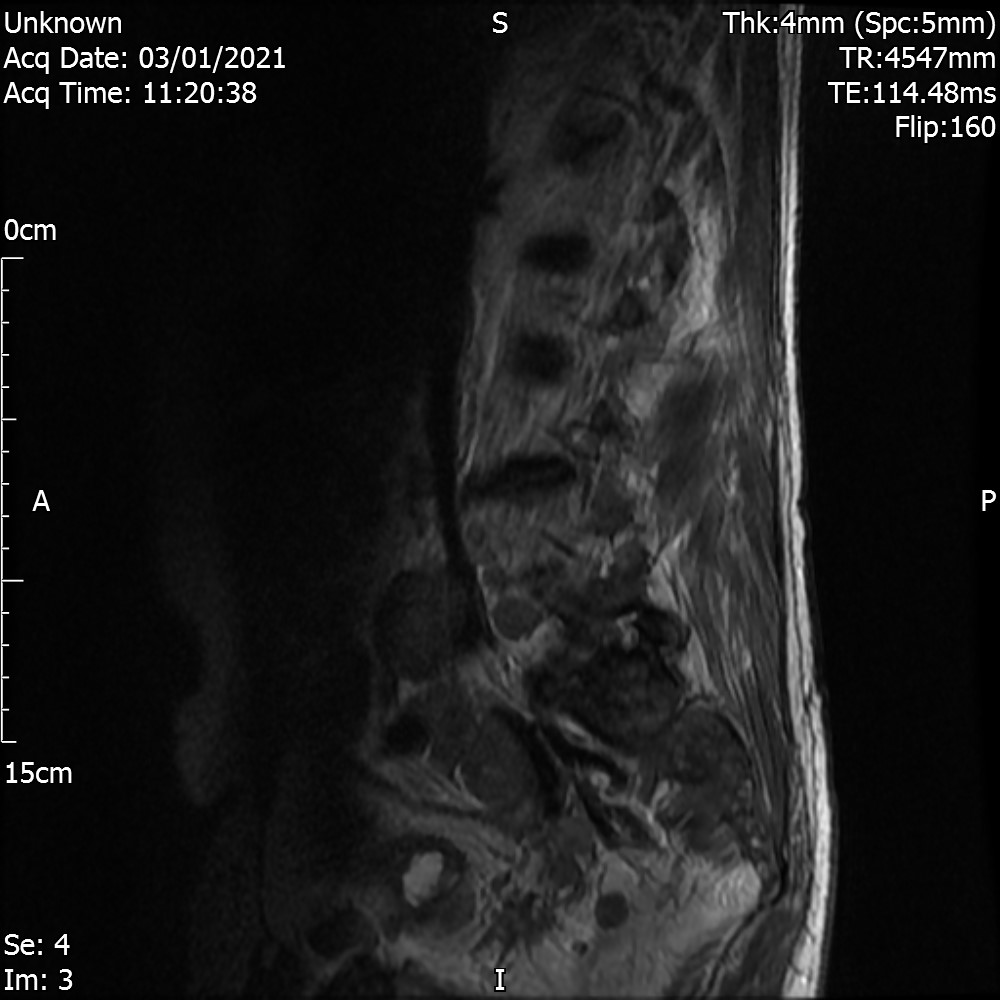
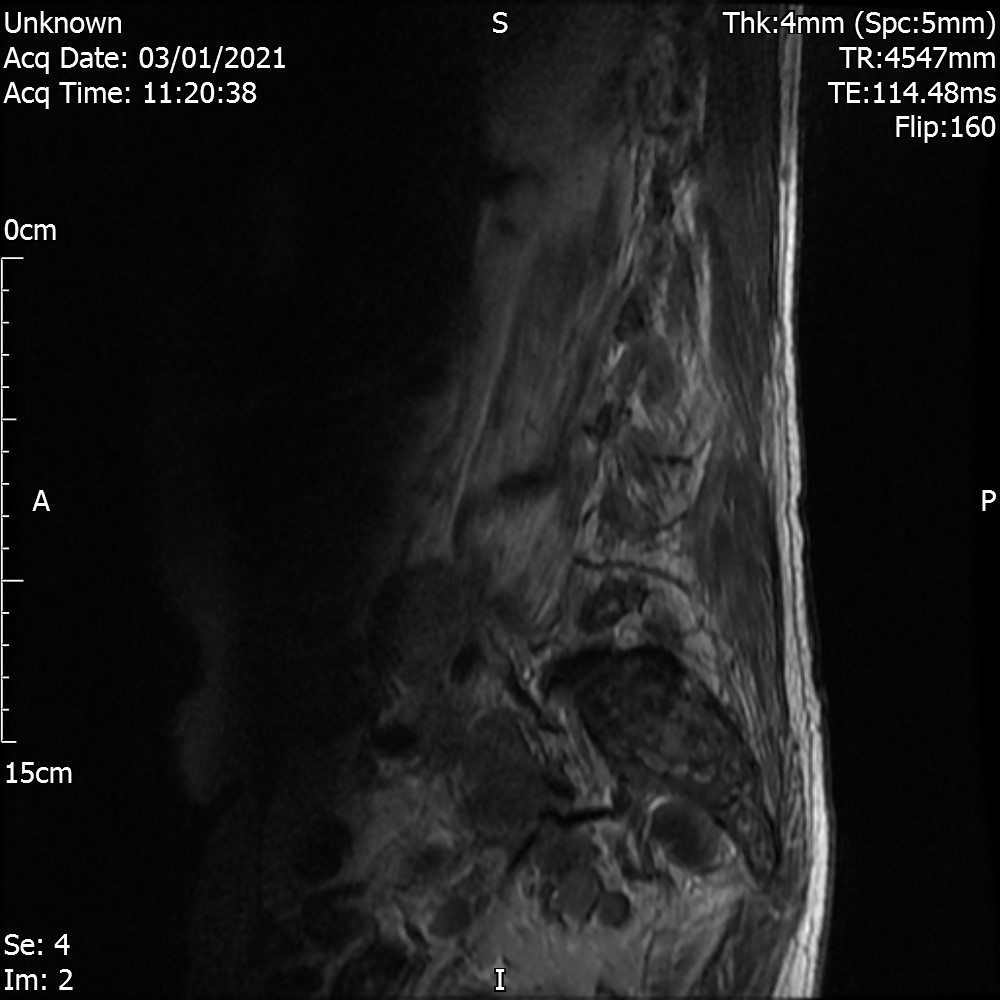
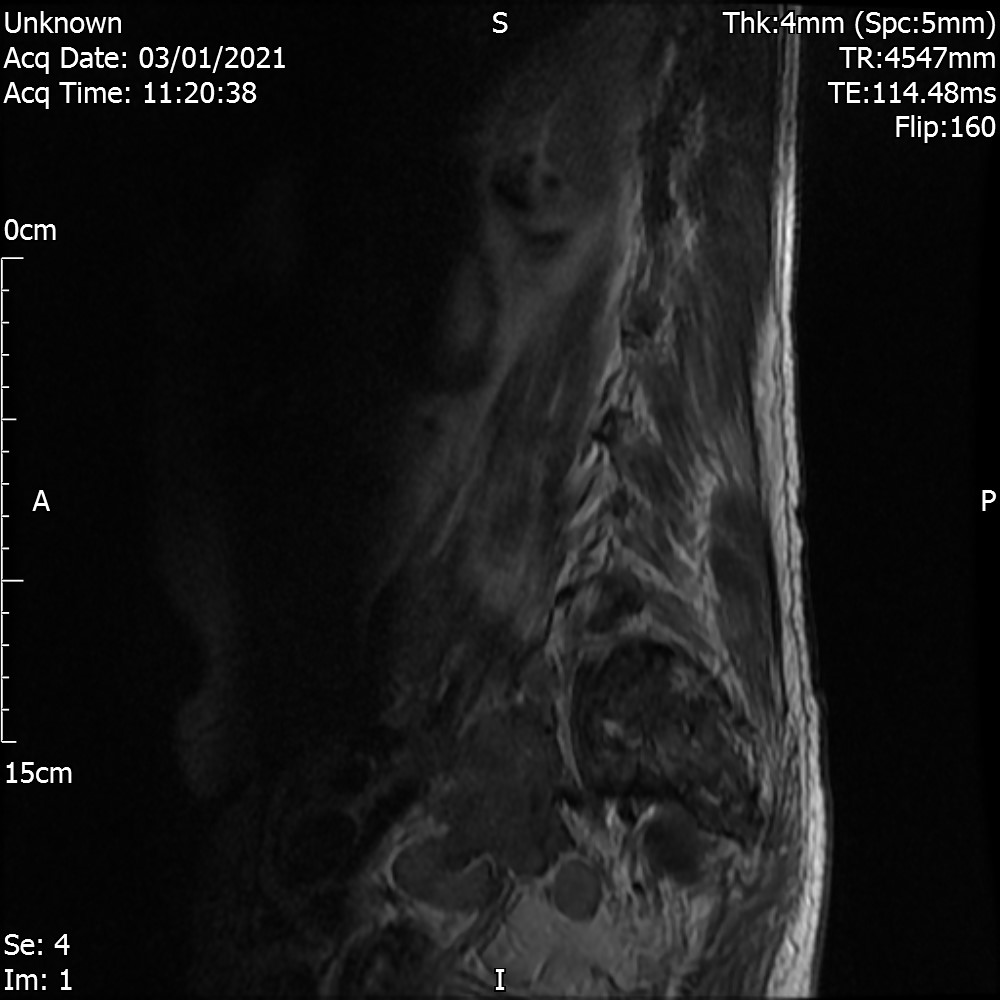
Lumbar Spine
Sagittal T2 view
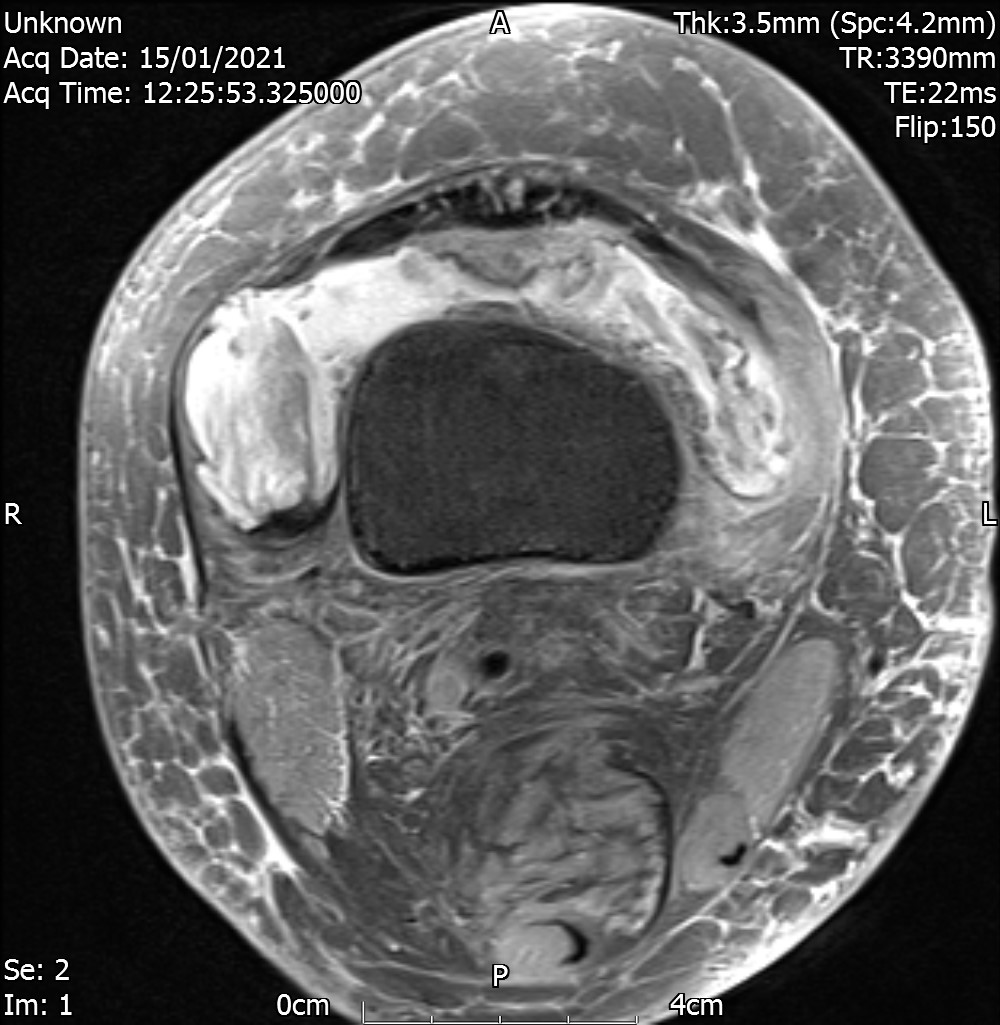
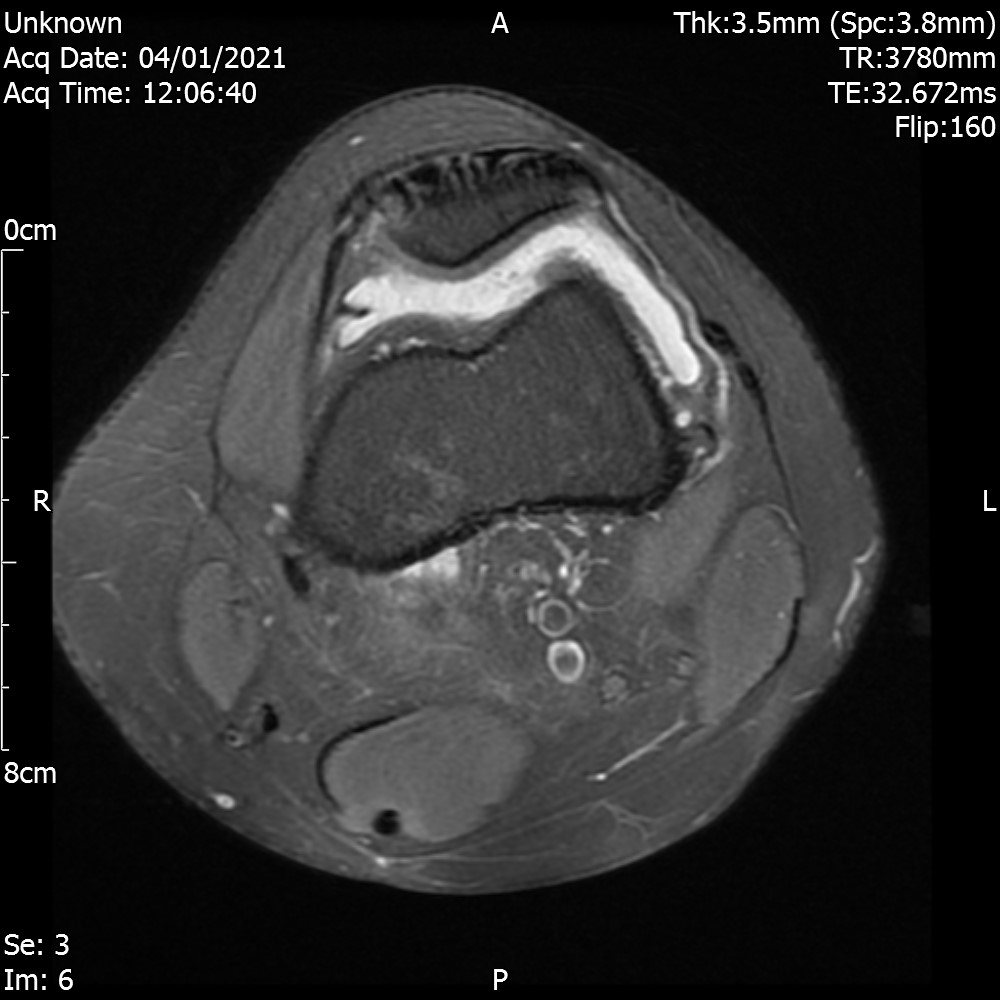
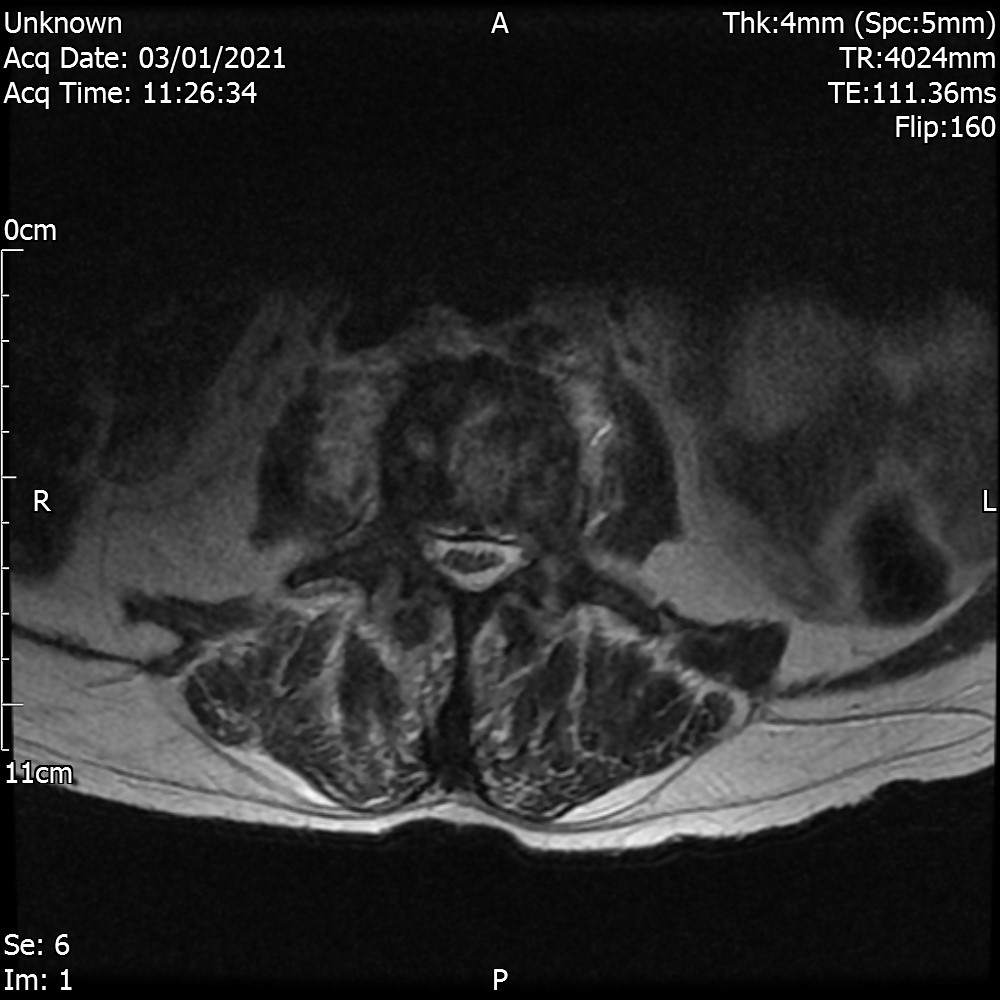
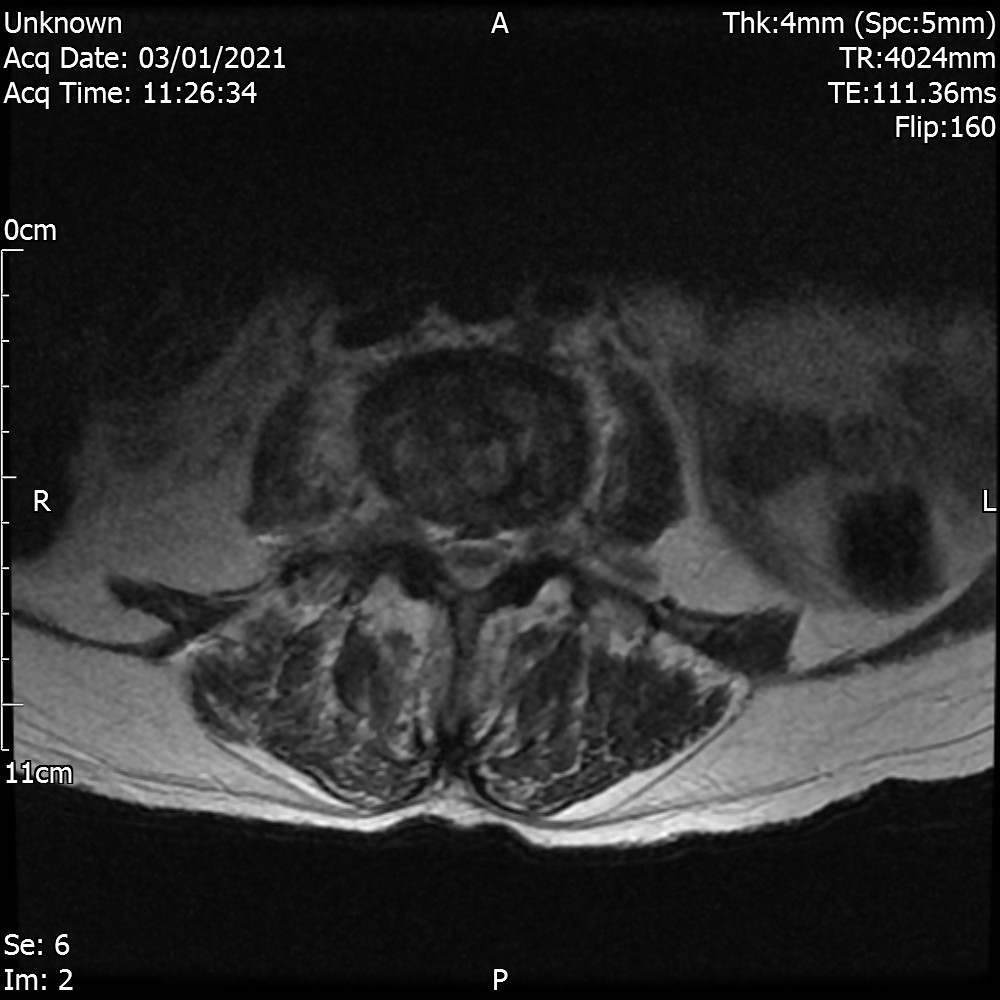
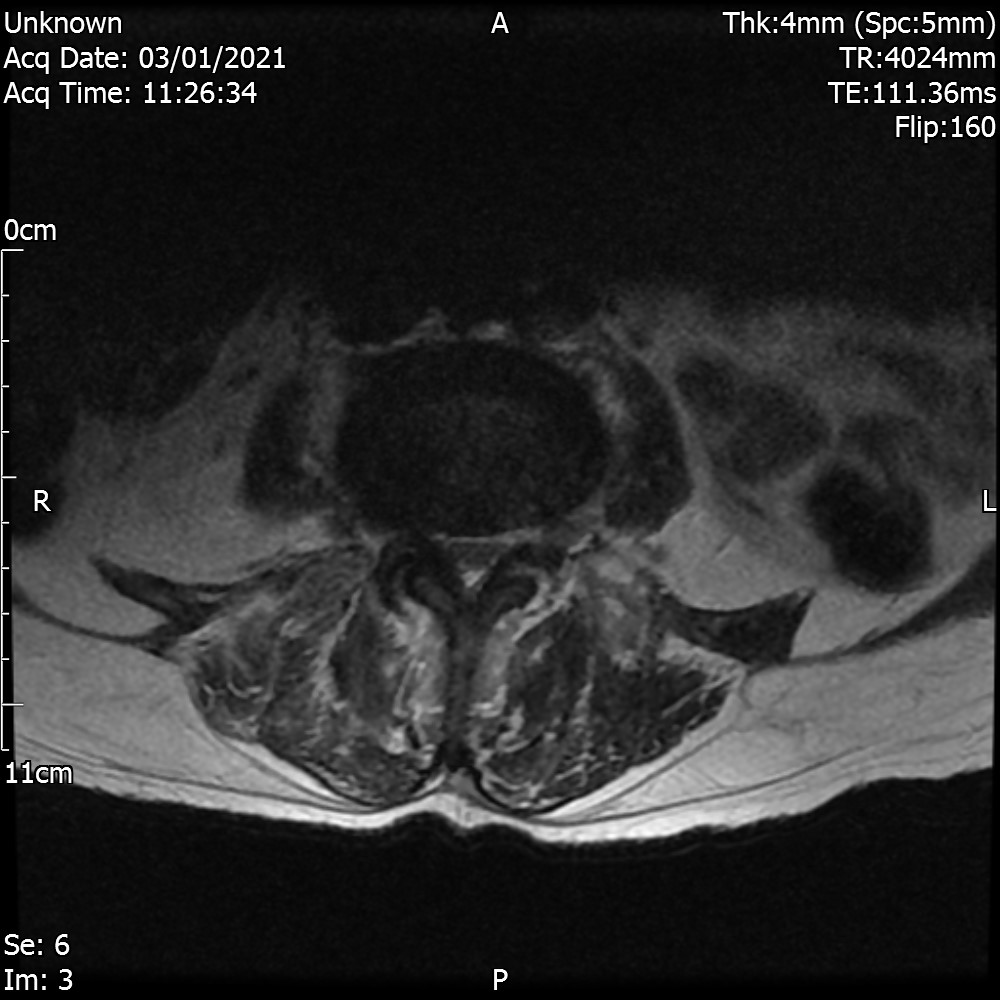
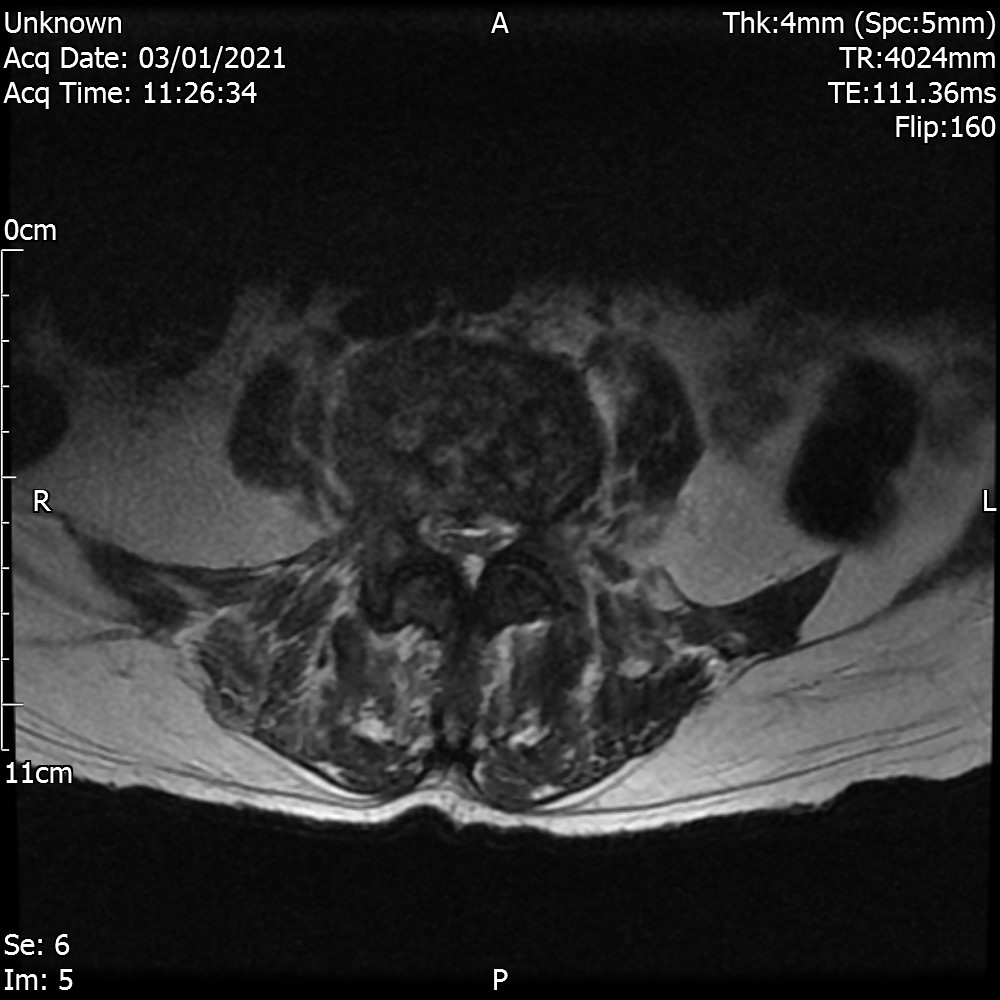
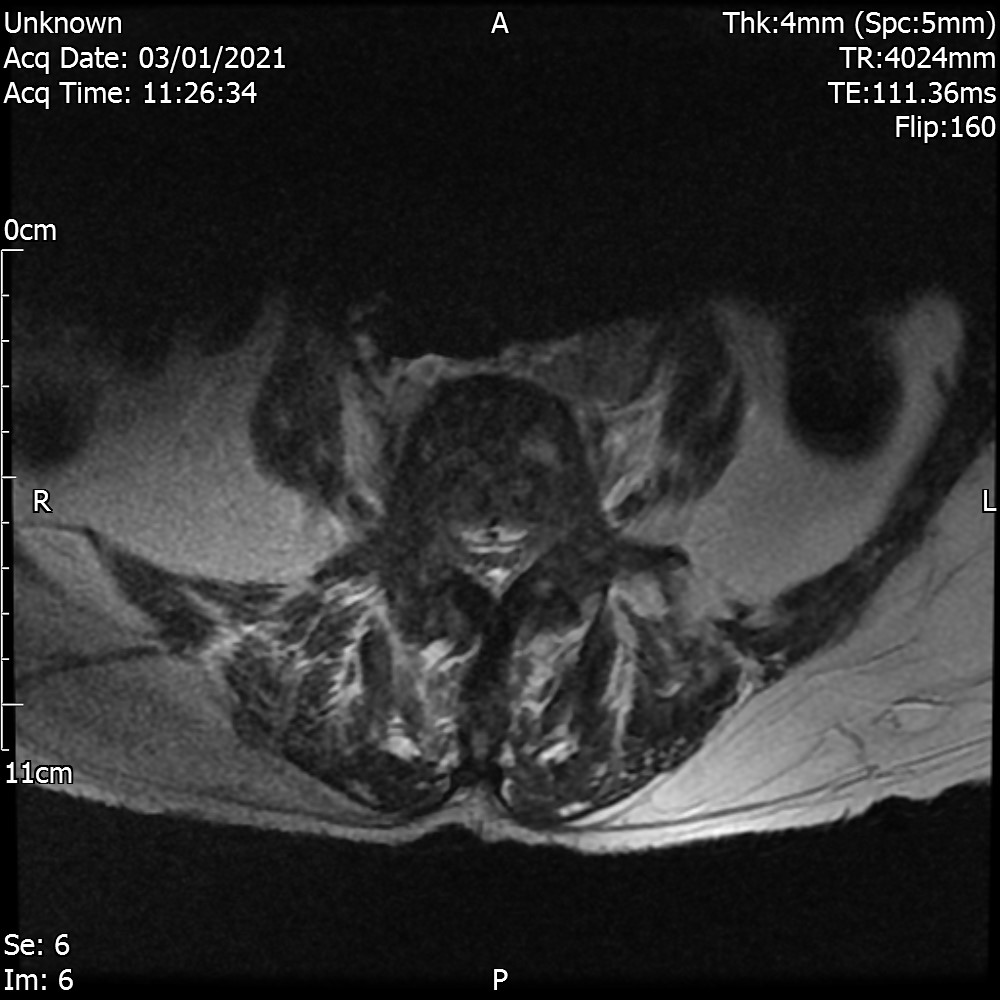
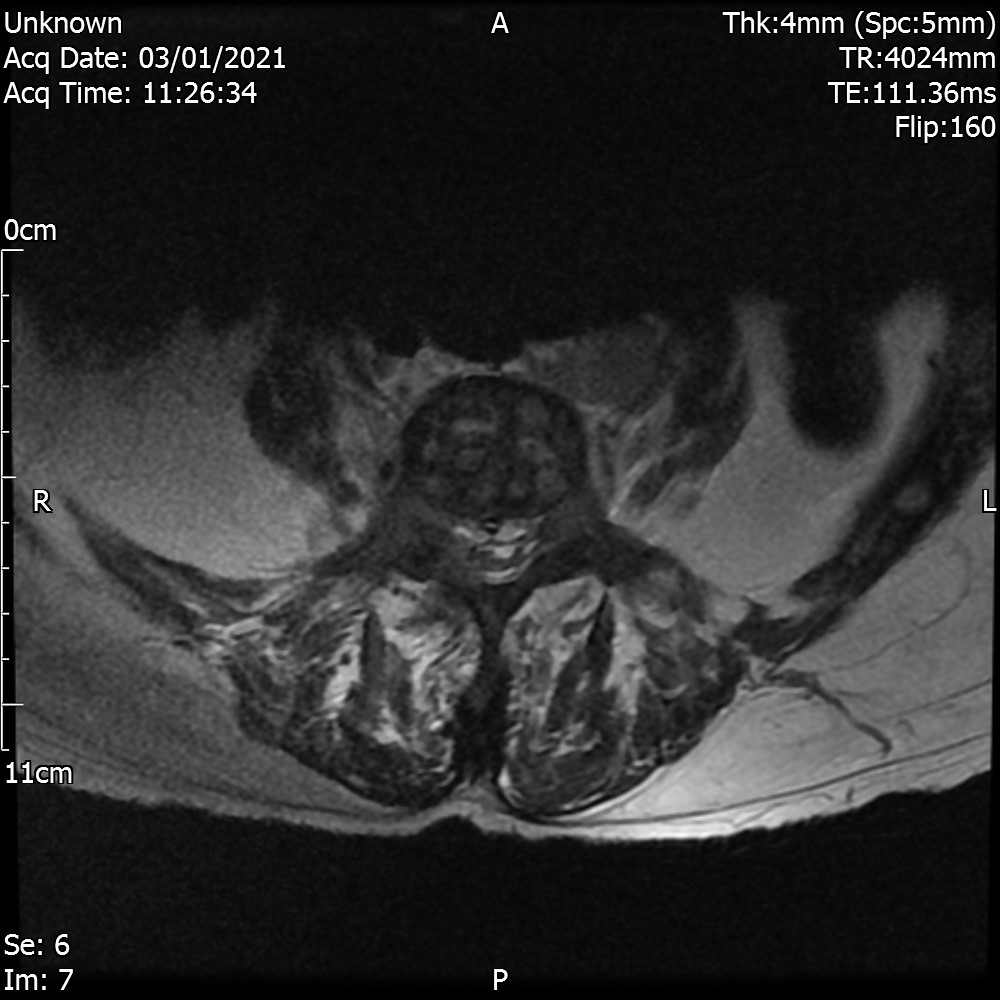
Axial T2 View

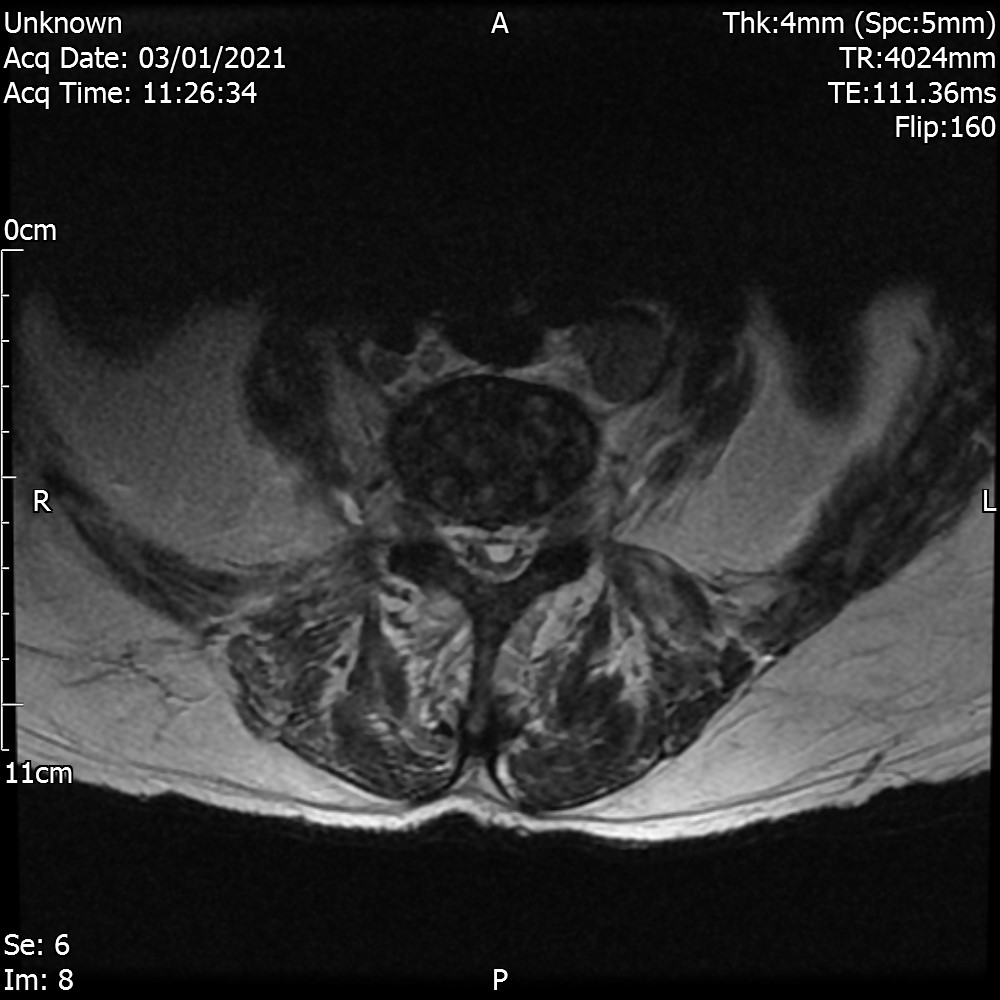
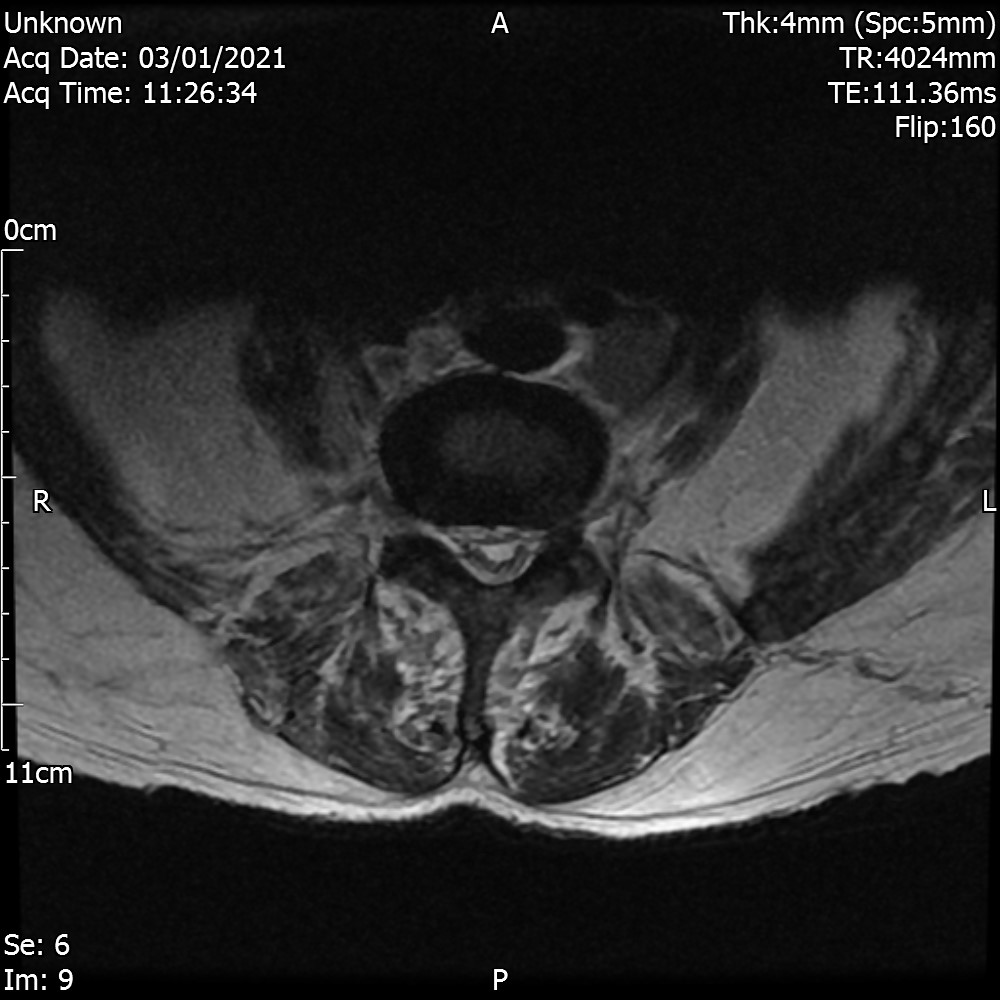
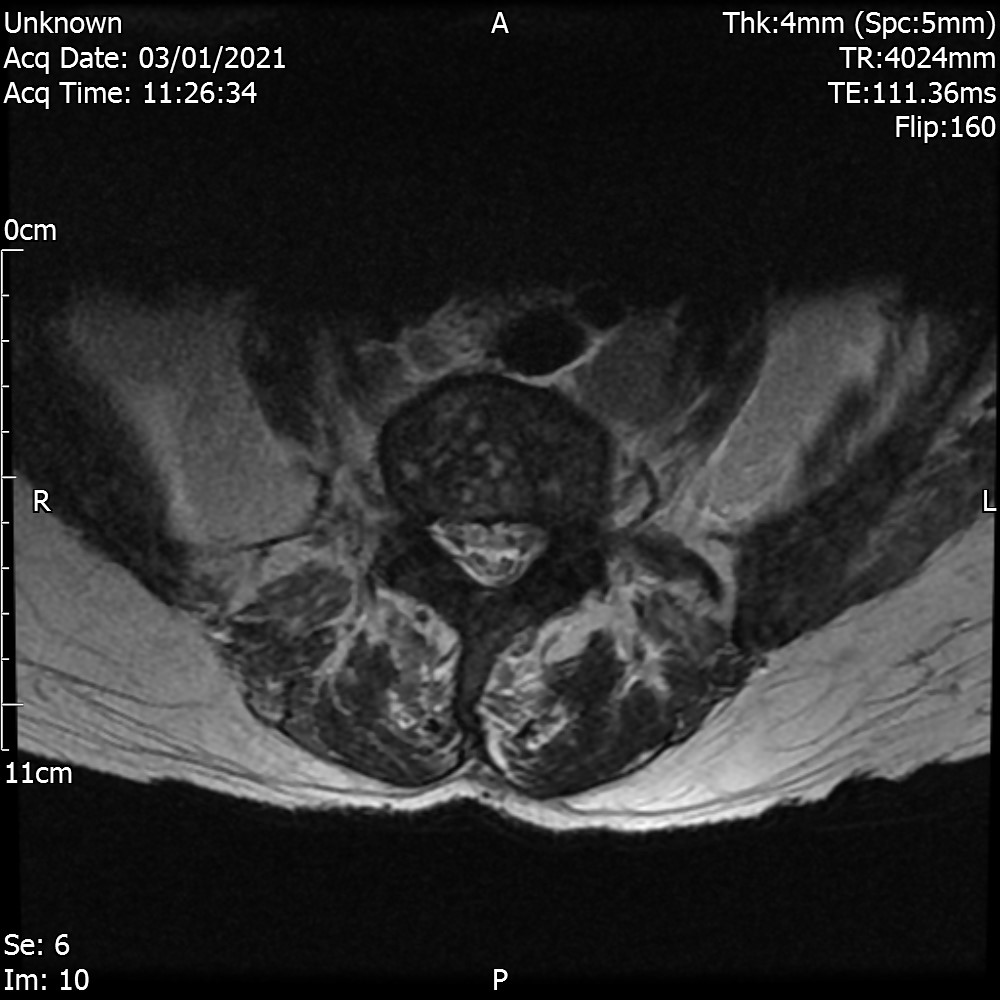
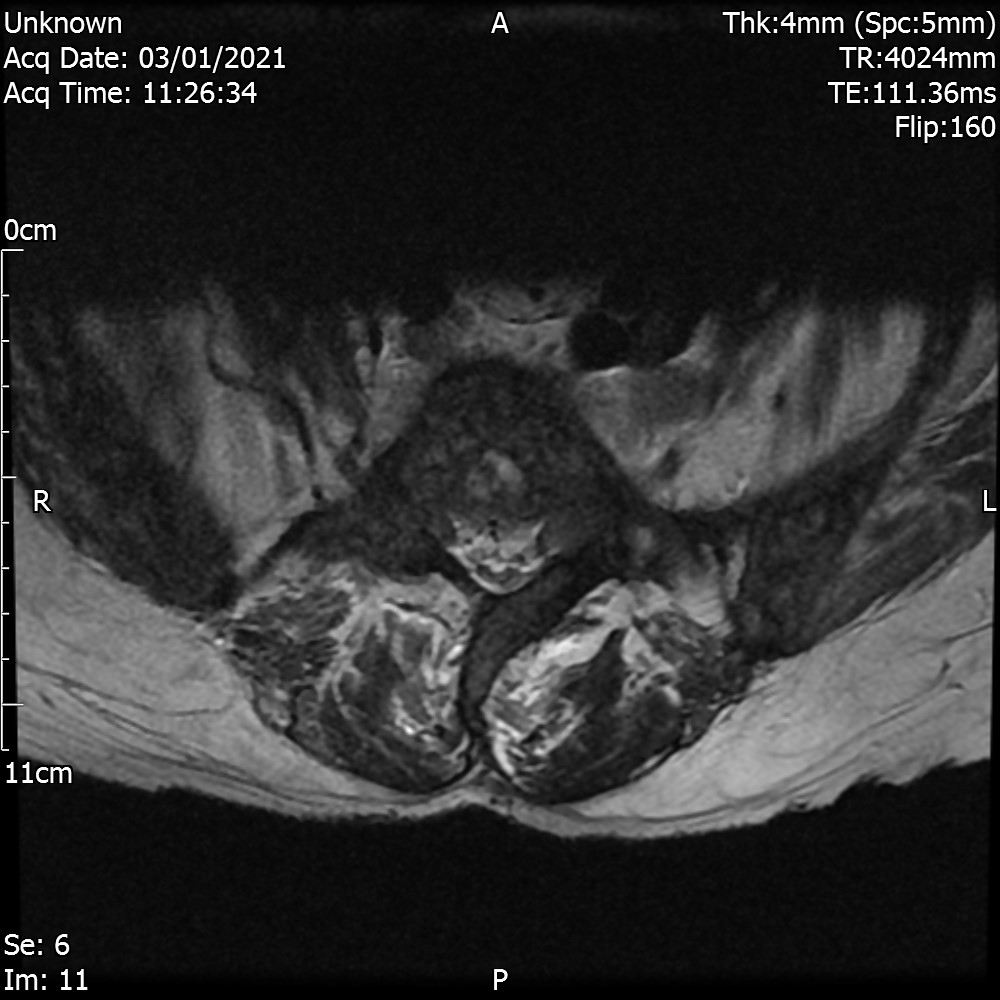


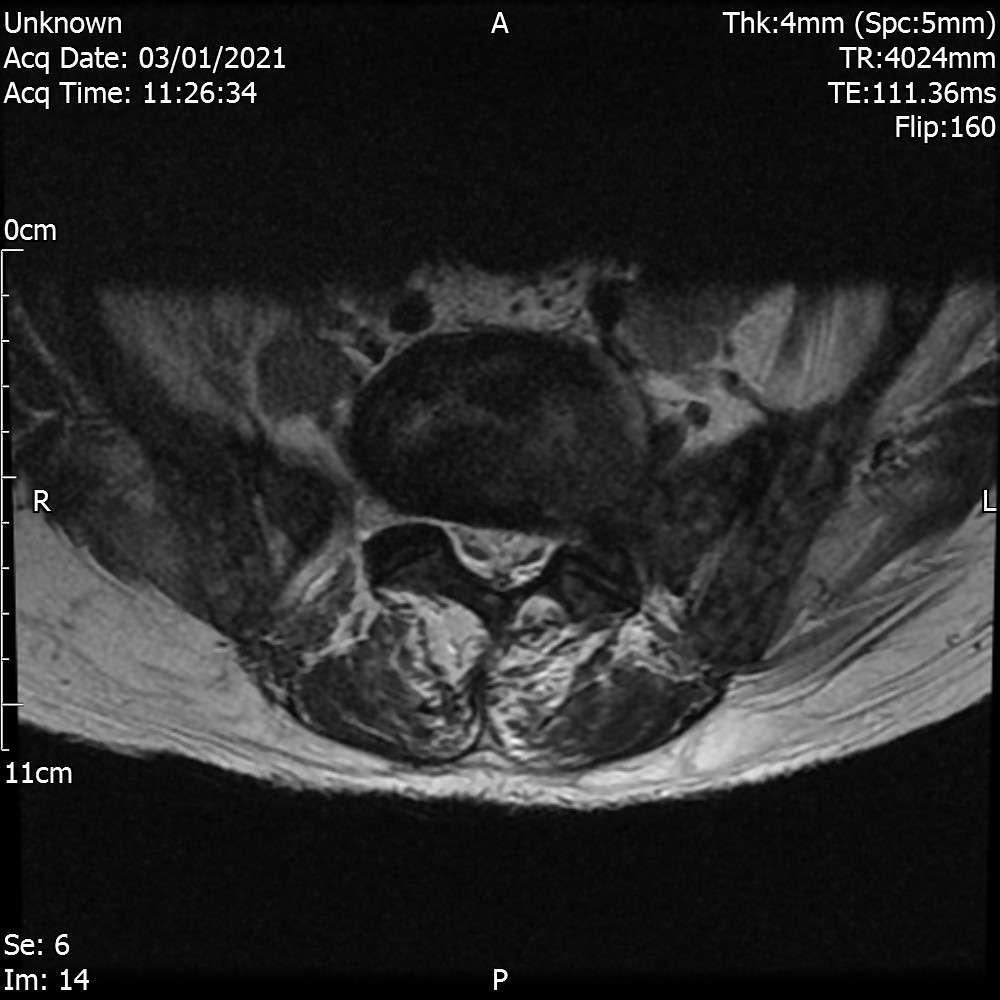
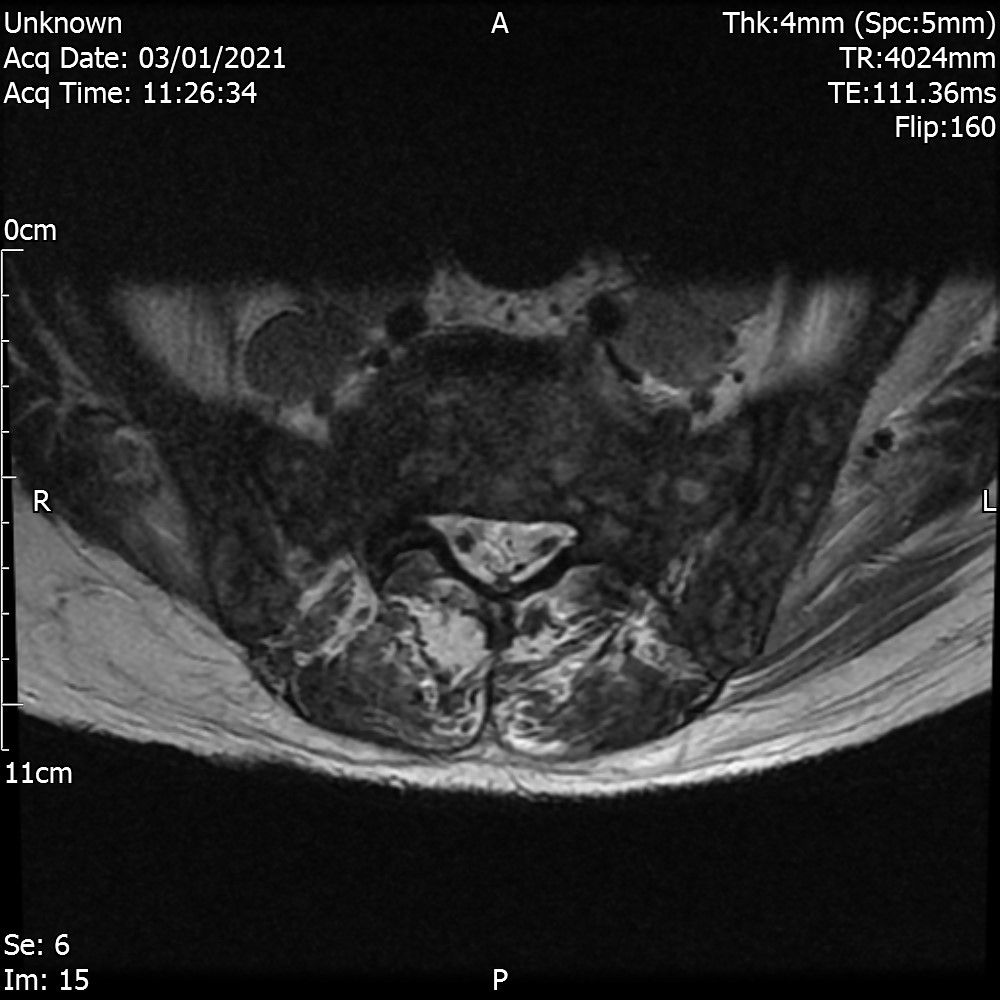
Sagittal T1 view
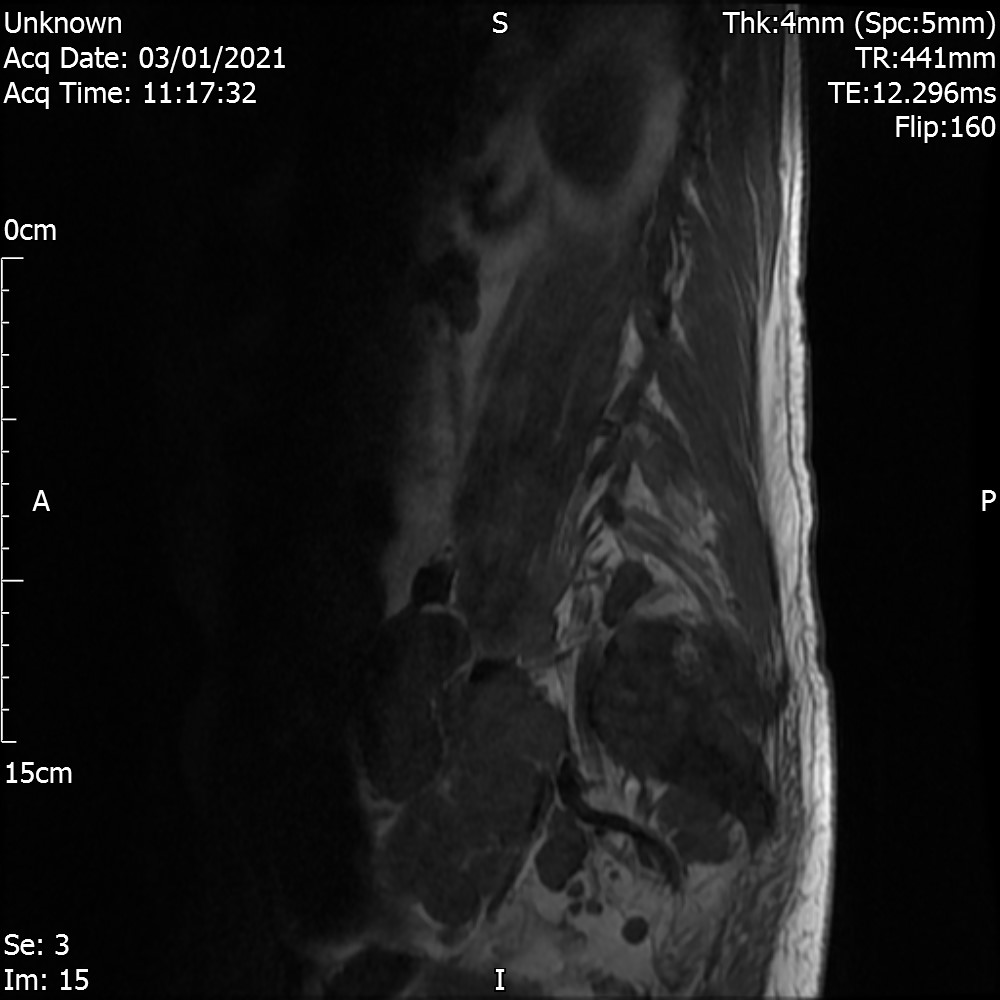
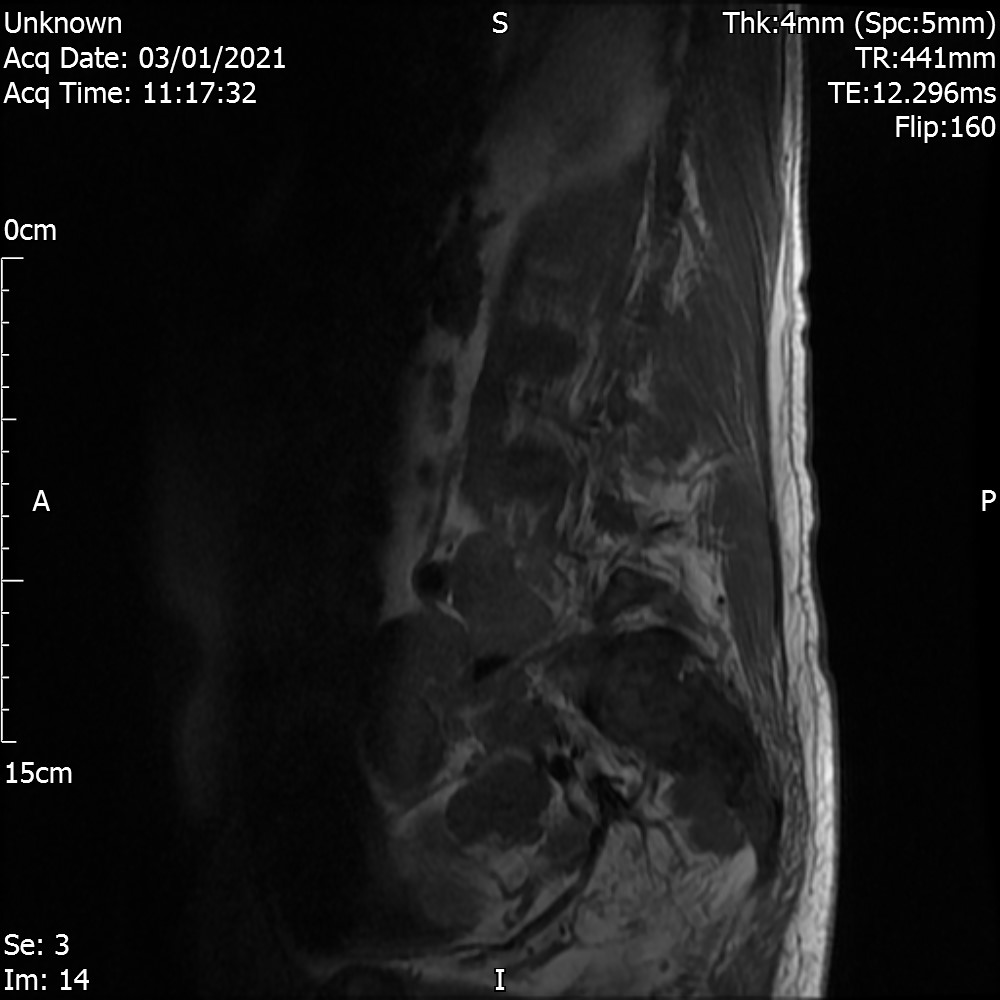

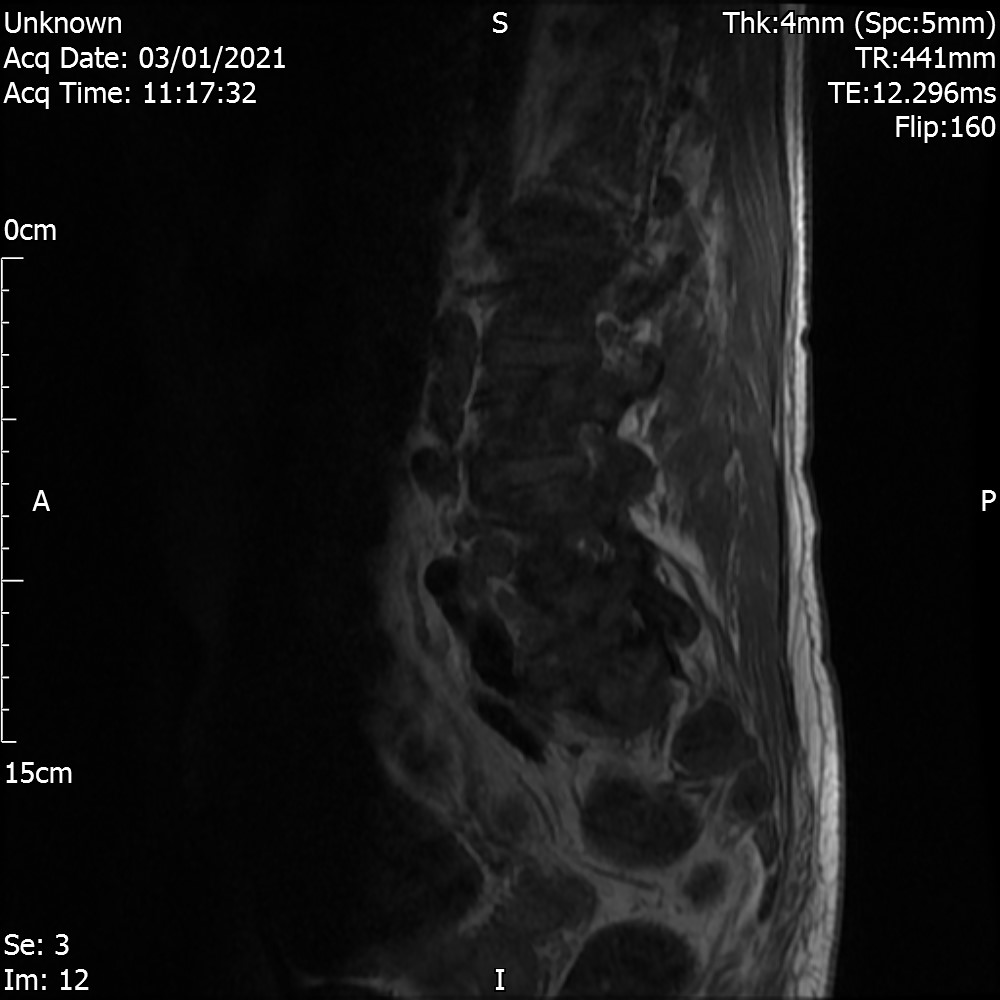
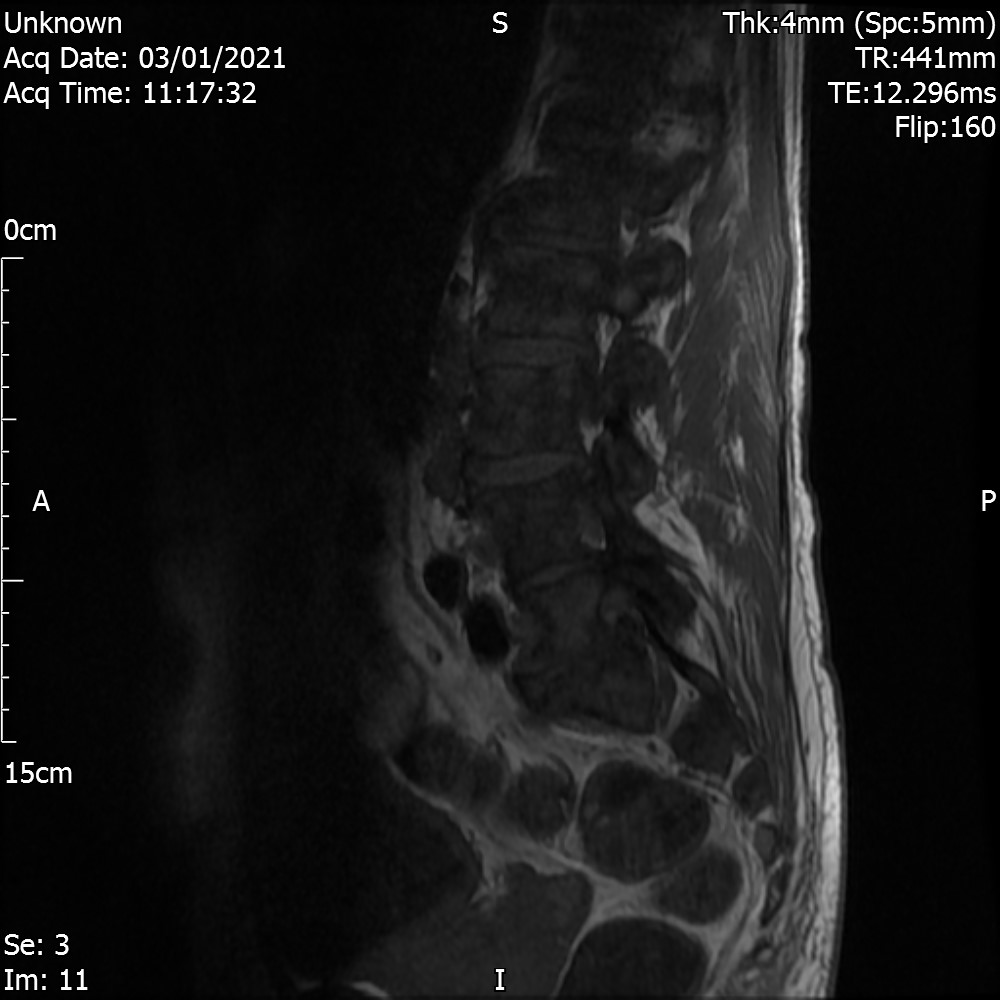
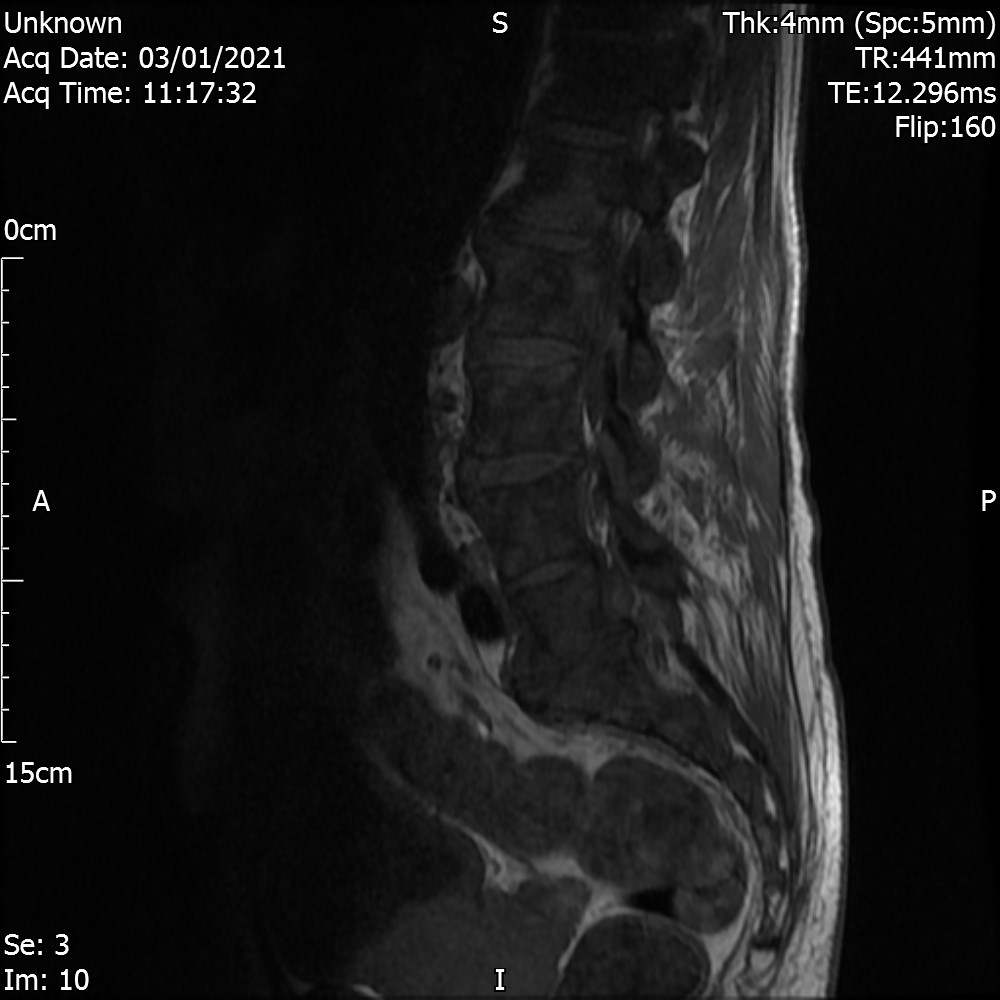

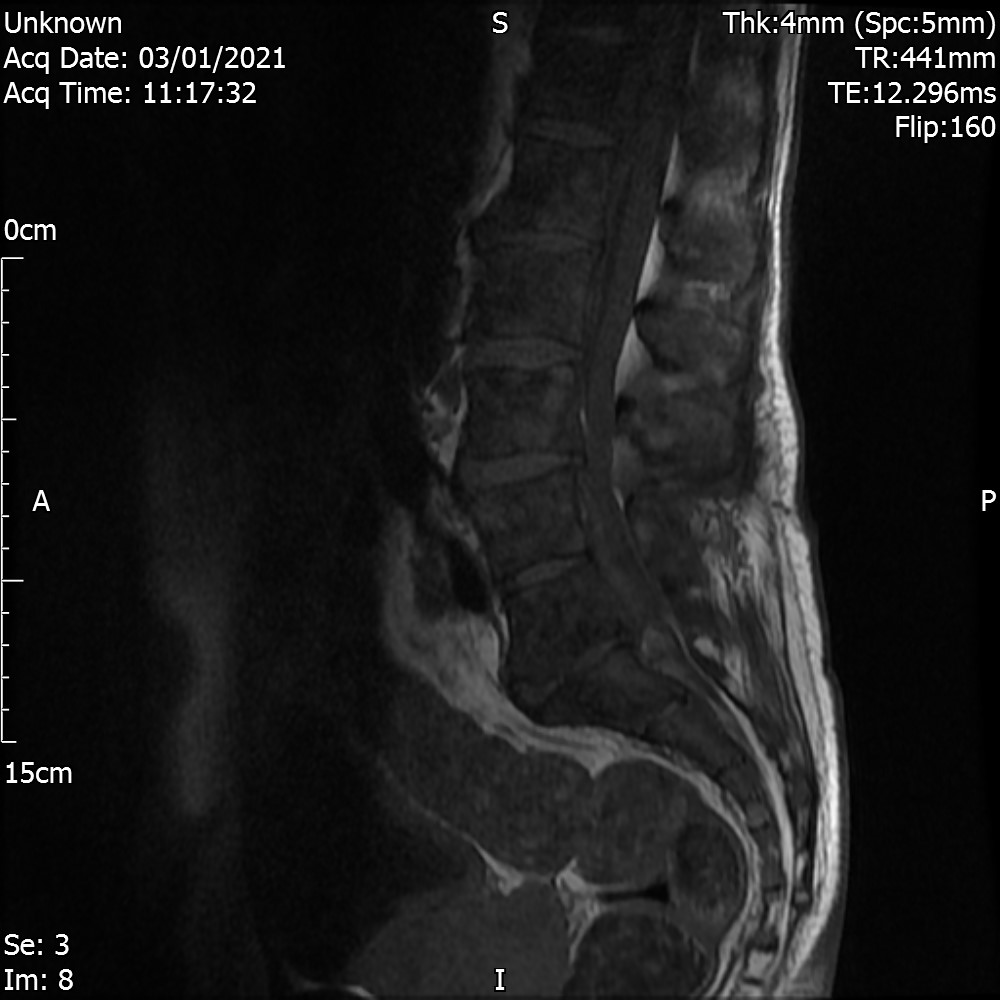

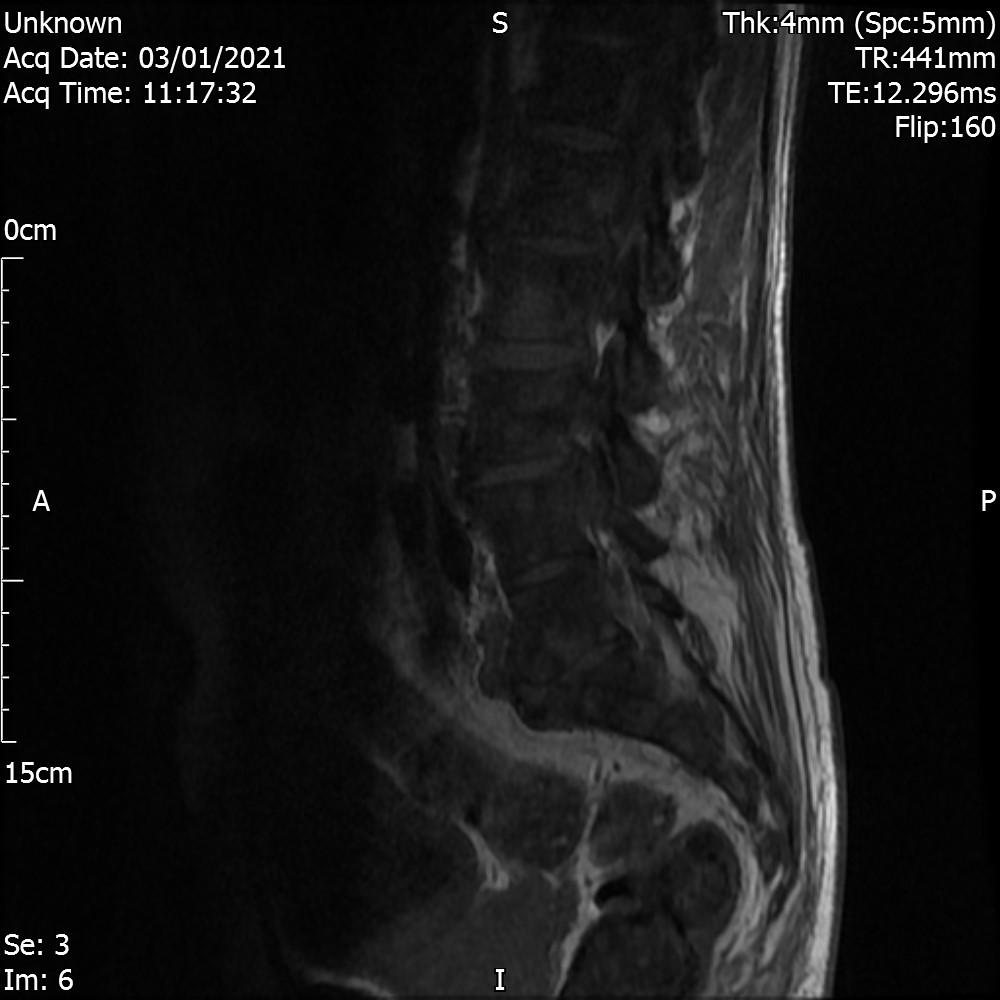
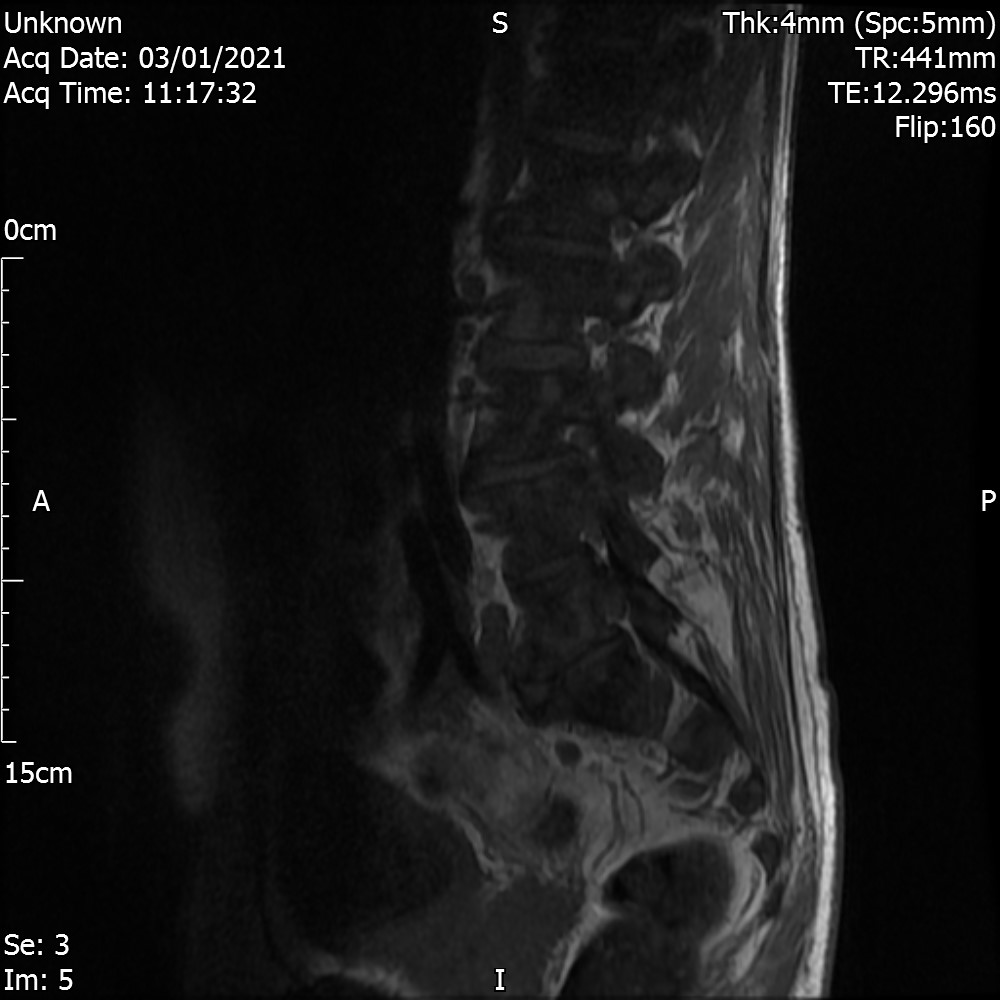
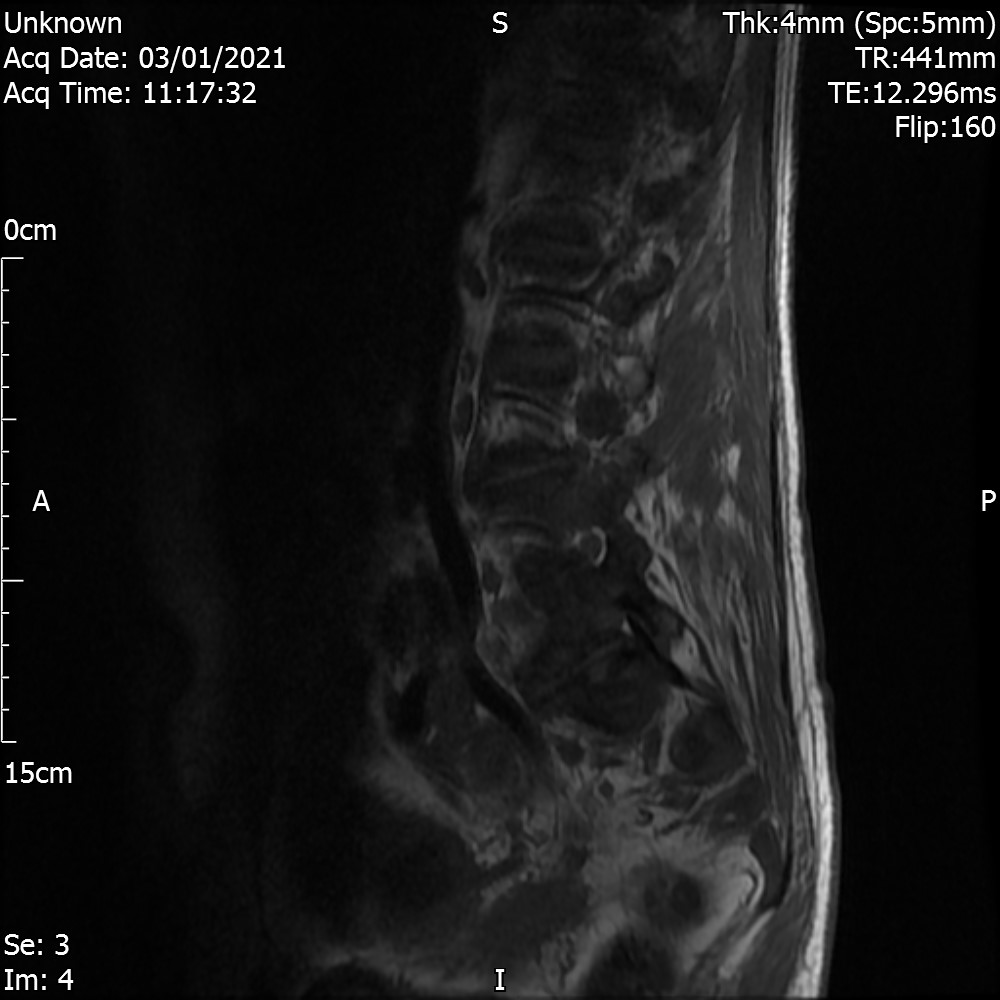
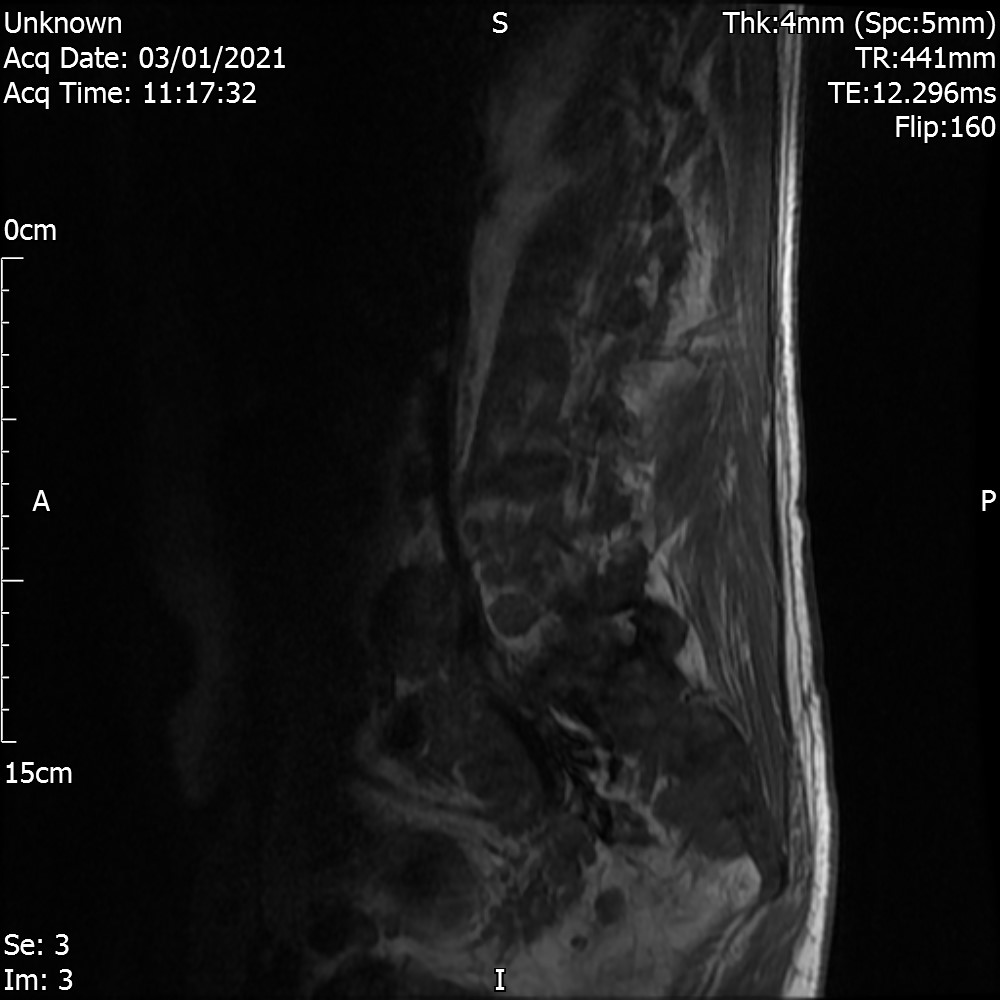
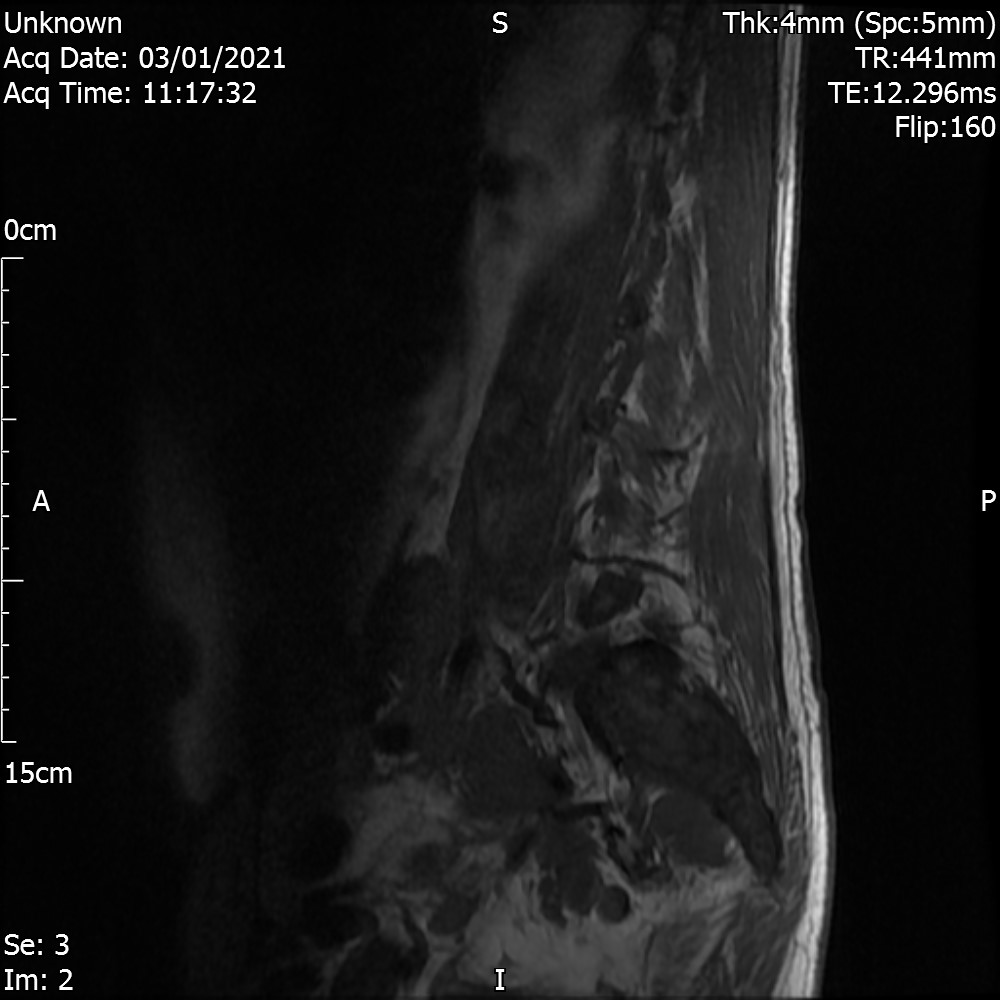
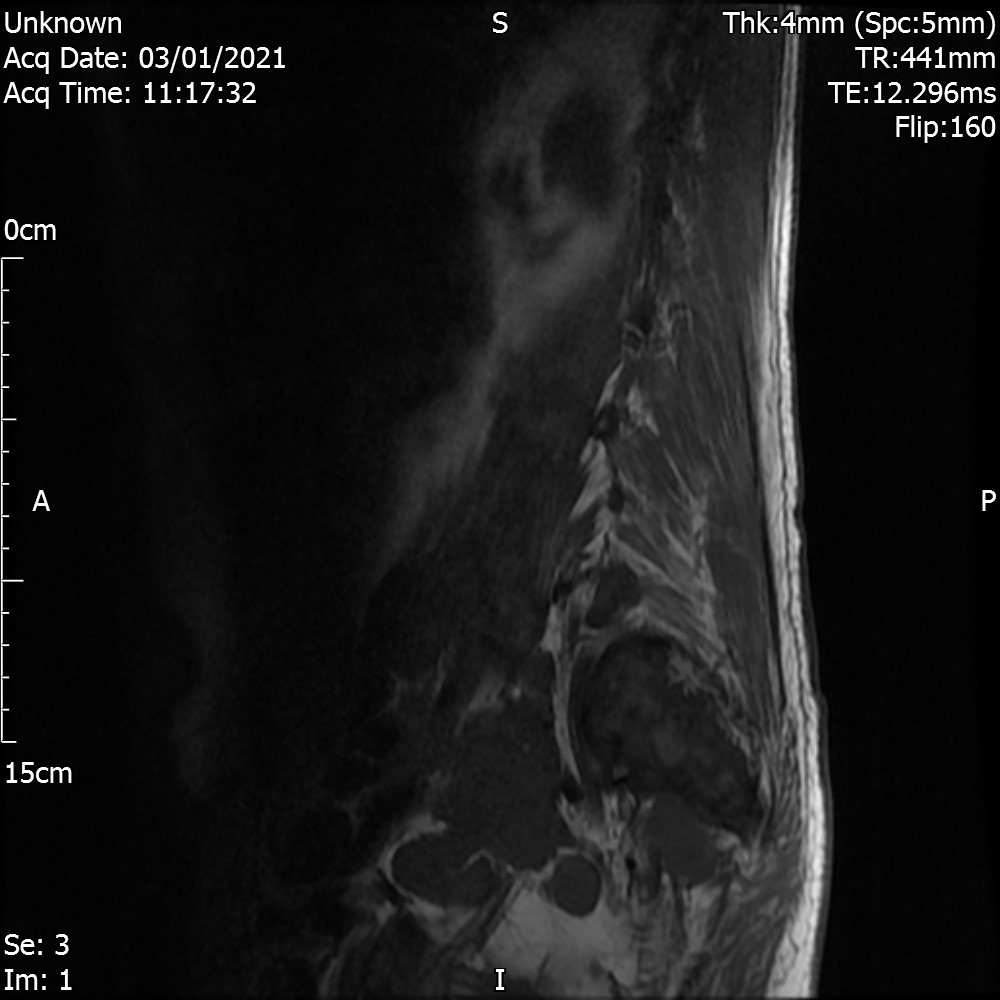
Study identifies multifocal abnormality of the anterior posterior coloumns consistent with metastatic bone disease.
In addition there is evidence of lower lumbar discopathy with circumferential narrowing of the L3-4 disc space which is associated with facet joint osteoarthropathy and mild narrowing of the canal and slight narrowing of the L4 Lateral recesses consistent with mild central canal stenosis.
At L4-5 disc level there is significant disc space narrowing. In addition there is loss of definition of the peridural and perineural fat planes in both the axial T2 and T1 images. This appearance is suspicious for extra-axial infiltration and epidural space infiltration by tumour. This is seen on the sagittal images with loss of the anterior epidural fat plane and loss of definition of the dural sac. This cannot be entirely attributed to movement artefact.
At L5-S1 there is eccentric disc bulge but not clearly compromising the thecal sac although there is some narrowing of the L5 neuroforamina and again the sagittal images show loss of perineural fat signal in the L5 canals which is likely due to soft tissue tumour infiltration.There is subtle nodularity to the lower thecal sac on the sagittal images which not entirely discounted the possibility of leptomeningeal deposition.
CONCLUSION
Extensive anterior posterior column metastatic bone disease. No direct vertebral expansion, compression or fracture.
At the lower lumbar levels there is suspicion of loss of perineural T1 fat signal possibly due to extradural tumour infiltration of the L4 and L5 foramina and the anterior epidural space. This is likely the explanation for symptoms. Subtle nodularity of the lower cauda equina is noted and this may be related to movement rather than definite leptomeningeal the position.
Outcome
patient was referred to Oncology under 2WW (2 week wait) pathway.
Red Flags
- Age
- Weight loss / loss of appetite
- Constant nature of pain
Analysis
30% of diagnosed bone metastasis have no known primary cancer. Lung, liver, pancreas and gastrointestinal tract are common sites for primary occult tumors. (Piccioli et al 2015).
The most likely visceral primary carcinomas to spread to the bone include those from the lungs, kidneys, prostate, breast and thyroid. (Carratero et al 2015)
Lung cancer is the most frequently identified primary tumour (25–67%) across all literature data (Argentiero et al 2019)
How are primary cancers diagnosed in SMUP?
- Radionuclide bone scanning
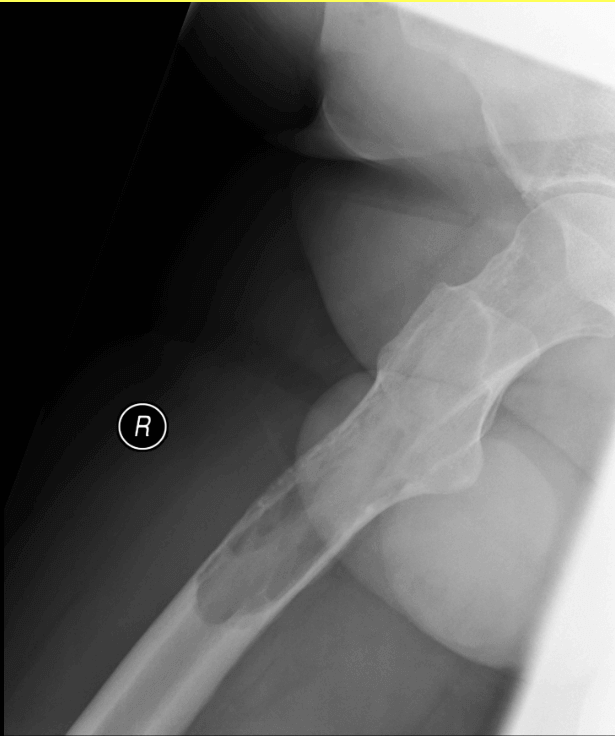
- Chest radiograph
- Abdominal ultrasound scan.
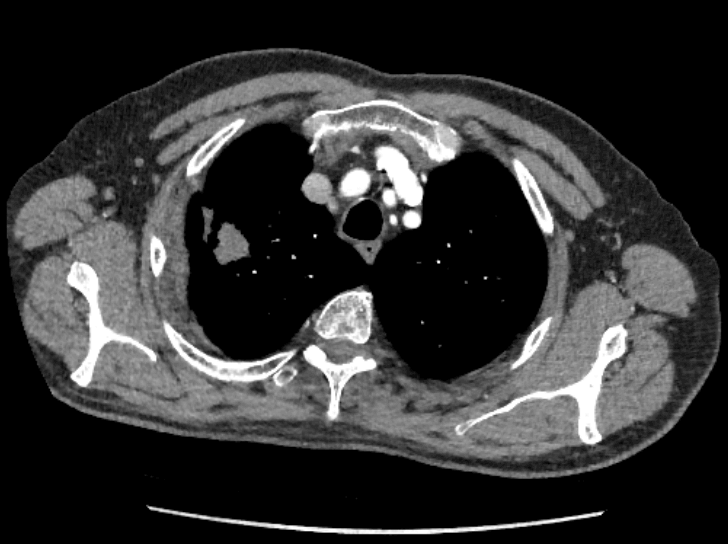
- Computed tomography (CT) of the chest and abdomen
- CT brain
- Tumour marker assays as clinically indicated (limited use in identifying primary with exception of PSA – Destombe et al 2007)
- Bone biopsy (usual sites – iliac bone, spine, sacrum, ribs) – can indicate site of primary cancer and histological type
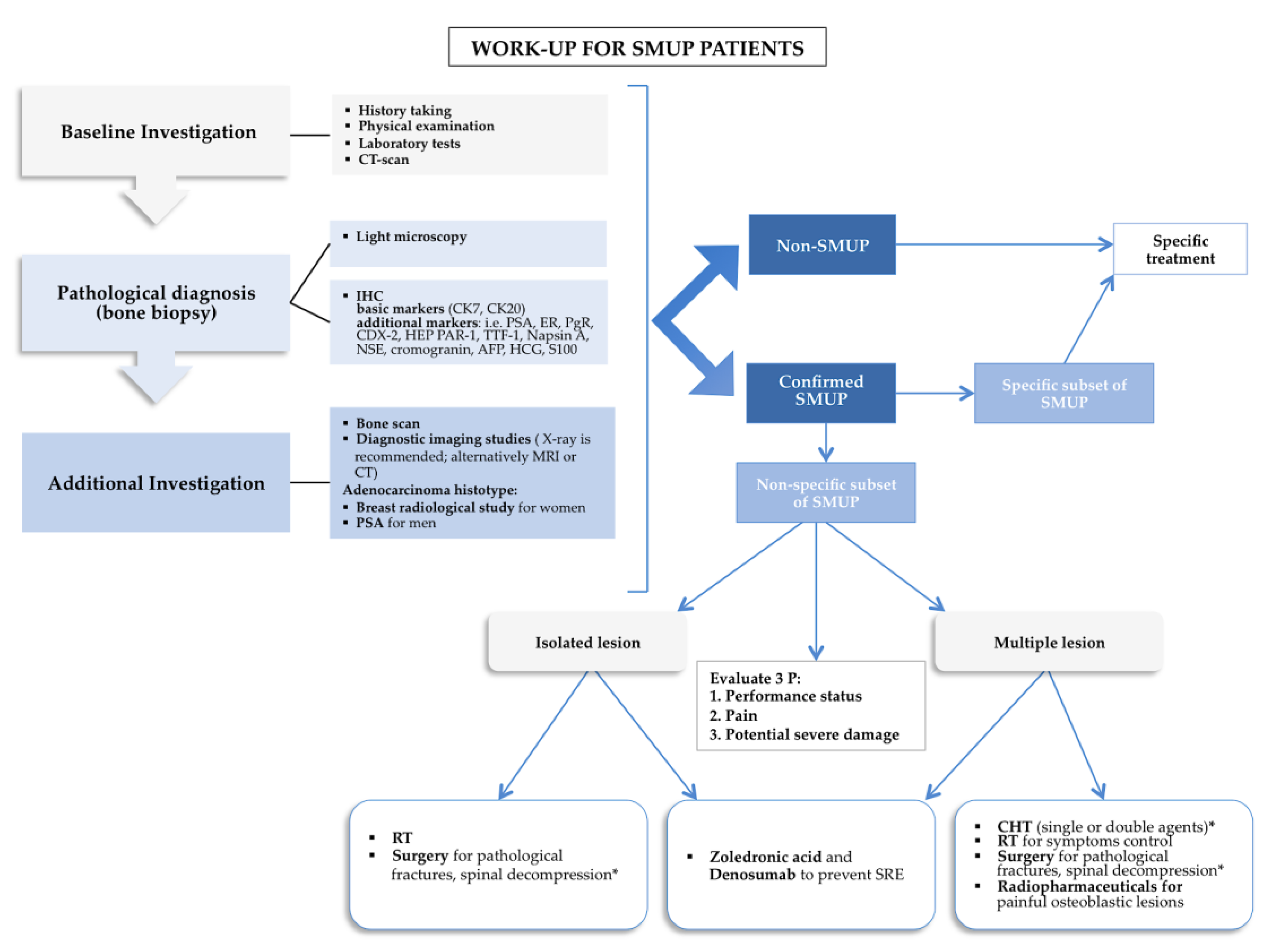
SMUP Flowchart by Argentiero et al 2019
References
- J Orthop Traumatol. 2015 Jun; 16(2): 81–86. Piccioli et al
- Joint Bone Spine 2007 Jan;74(1):85-9. doi: 10.1016/j.jbspin.2006.05.009
- Unknown primary tumors – Natoli et al 2011
- Primary bone metastasis as first manifestation of an unknown primary tumour – Carratero el al 2015 (BMJ Case report)
- Skeletal Metastases of Unknown Primary: Biological Landscape and Clinical Overview – Argentiero et al 2019 (Cancers)
- A mini review on cancer of unknown primary site: A clinical puzzle for the oncologists – Pavlidis et al 2015 (Journal of Advanced Research)